







If you ask glaucoma patients to describe their vision, very rarely will you hear them describe a scotoma. Even when glaucoma patients have scotomas on visual field testing, the most common patient responses to that question are “my vision is blurred,” and “I need more light to see well.”1 Most patients who have lost vision from glaucoma are describing issues that are the result of worsening contrast sensitivity. This creates an inherent disconnect with patients as a doctor may show a patient a visual field printout with a deficit such as a nasal step, but the patient does not see anything like that. For years, patient education brochures have illustrated how glaucoma damages vision by showing a picture with everything black except for a clear center. These illustrations did a disservice to doctors and patients, because that is not what glaucoma patients see.1 How can patients truly understand the importance of glaucoma treatment if the visual deficit that is explained to them is not something they can relate to?
Contrast sensitivity is one of the most important aspects of vision in terms of how well people function in their daily lives. This includes people with glaucoma and other eye problems. Our group previously tested glaucoma patients’ ability to perform visually related daily activities and compared their visual performance scores to visual fields, visual acuity, optic nerve damage, intraocular pressure, stereopsis, and contrast sensitivity. Contrast sensitivity scores were the best predictor of how well glaucoma patients could perform visually related daily tasks — far superior to visual fields.2
Contrast sensitivity evaluates how well a person can distinguish an object from its background. If a large amount of contrast is needed to identify an object from its background, then the contrast sensitivity is poor. If someone can distinguish very subtle differences in the luminance of an object from the luminance of its background, then their contrast sensitivity is high. Several factors influence people’s ability to discern contrast. One of those factors is the size of what they are viewing. The larger the object, the more easily it is seen. A car is easier to see than a golf ball and would need less contrast than a golf ball to be visible. Another aspect is the difference in brightness between the object and its background. For example, a large, black car is difficult to see on a dark night, but a small, white golf ball is easily seen during the day against the background of dark green grass. People with ocular disease that diminishes the ability to see contrast (that is, they have poor contrast sensitivity) will have a decreased ability to see well as the light gets dimmer, as at the end of the day. Thus, at night, when there are low levels of light, the demand for good low spatial frequency contrast sensitivity may be beyond the visual capacity of a diseased eye, whereas a person with a healthy eye would see the object. This may partially explain the higher incidence of car accidents and falls in glaucoma patients.3
Many contrast sensitivity tests have been developed, though none thus far have become commonly accepted in clinical practice. One reason for this is the lack of recognition that seeing contrast is the best predictive indicator of what a person can see. Furthermore, the correlation between Snellen visual acuity and the ability to read is so apparent, and the importance of reading is so apparent, that a physician may incorrectly believe visual acuity to be a more useful measure than contrast sensitivity. Few ophthalmologists know that the correlation between contrast sensitivity and reading is better. Additionally, methods of assessing visual acuity have been used for hundreds of years, the result being they have become habitual and their clinical value is understood, whereas testing for contrast sensitivity is not routine and its results are of uncertain clinical meaning to most ophthalmologists. Another impediment to the use of testing contrast sensitivity is the way its scores are reported. For example, a visual acuity of 20/40 is much easier to understand than a log contrast sensitivity score of 1.50.
Contrast Sensitivity Tests
Contrast sensitivity tests are categorized into 2 groups: those using letters and those using gratings. There are benefits and drawbacks of evaluating contrast sensitivity with each method, but the most important aspects of a test are how well it can identify healthy from diseased eyes and how reproducible the results are.4 Many contrast sensitivity tests with gratings have been developed, though most have low test-retest reproducibility.5-7
The letter-based contrast sensitivity tests, such as the Pelli-Robson chart, often have better reproducibility, but can be influenced by literacy and chart fading.8 Nevertheless, numerous studies have shown that contrast sensitivity is diminished in glaucoma.2,9-12
Development of the SPARCS Test
We developed and patented the Spaeth-Richman Contrast Sensitivity Test (SPARCS) with the goal of identifying people with ocular disease, monitoring progression, generating reproducible results, and providing easy access to the test. SPARCS is accessed via http://www.sparcscontrastcenter.com and assesses both central and peripheral contrast sensitivity using gratings of varying levels of contrast. There is both a quick screening version of SPARCS and a more comprehensive version of SPARCS available on the website. Although the test uses traditional log-based Weber contrast, the total score is converted to a scale out of 100 for an easier understanding of the result.
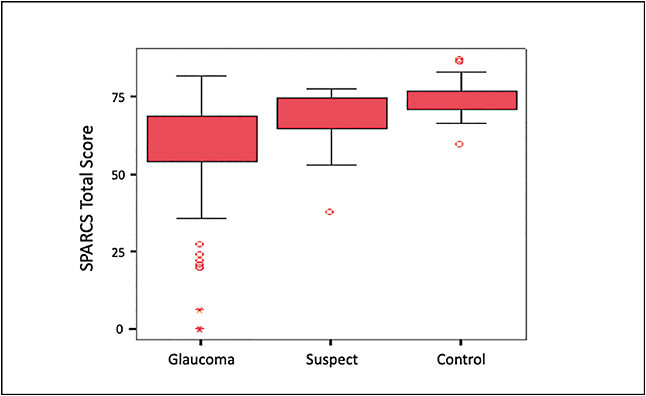
A total SPARCS score of less than 70 has been shown to have 80% sensitivity and 93% specificity for glaucoma. If a glaucoma patient had some loss of rim tissue on optic nerve examination, the SPARCS score was lower than controls’ SPARCS scores 95% of the time. In one of our studies with a wide severity of glaucomatous damage, the average glaucoma patients’ SPARCS score was 59, the average glaucoma suspect score was 69, and the average control score was 74. As with other tests for glaucoma, however, there is some overlap between normal, glaucoma suspects, and glaucoma patients (Figure 1). Some individuals with minimal optic nerve damage still score well.13
Future Use of Contrast Sensitivity Testing
SPARCS has been involved as a visual assessment for numerous clinical trials, many from our group and some from international studies. Most of the studies have been in a traditional clinical or research setting. The true potential of SPARCS may, however, not be realized in a doctor’s office, but in a person’s home. This offers a way to follow visual loss more closely and more affordably than is now possible. GP
References
- Hu CX, Zangalli C, Hsieh M, et al. What do patients with glaucoma see? Visual symptoms reported by patients with glaucoma. Am J Med Sci. 2014;348(5):403-409.
- Richman J, Lorenzana LL, Lankaranian D, et al. Importance of visual acuity and contrast sensitivity in patients with glaucoma. Arch Ophthalmol. 2010;128(12):1576-1582.
- Haymes SA, Leblanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Risk of falls and motor vehicle collisions in glaucoma. Invest Ophthalmol Vis Sci. 2007;48(3):1149-1155.
- Richman J, Spaeth GL, Wirostko B. Contrast sensitivity basics and a critique of currently available tests. J Cataract Refract Surg. 2013;39(7):1100-1106.
- Jones HS, Moseley MJ, Thompson JR. Reliability of the Cambridge low contrast gratings. Ophthalmic Physiol Opt. 1994;14(3):287-289.
- Reeves BC, Wood JM, Hill AR. Vistech VCTS 6500 charts—within- and between-session reliability. Optom Vis Sci. 1991;68(9):728-737.
- Pesudovs K, Hazel CA, Doran RM, Elliott DB. The usefulness of Vistech and FACT contrast sensitivity charts for cataract and refractive surgery outcomes research. Br J Ophthalmol. 2004;88(1):11-16.
- Haymes S, Roberts K, Cruess A, et al. The letter contrast sensitivity test: clinical evaluation of a new design. Invest Ophthalmol Vis Sci. 2006;47(6):2739-2745.
- Lahav K, Levkovitch-Verbin H, Belkin M, Glovinsky Y, Polat U. Reduced mesopic and photopic foveal contrast sensitivity in glaucoma. Arch Ophthalmol. 2011;129(1):16-22.
- Onal S, Yenice O, Cakir S, Temel A. FACT contrast sensitivity as a diagnostic tool in glaucoma: FACT contrast sensitivity in glaucoma. Int Ophthalmol. 2008;28:407-412.
- Sample PA, Juang PS, Weinreb RN. Isolating the effects of primary open-angle glaucoma and the contrast sensitivity function. Am J Ophthalmol. 1991;112(3):308-316.
- Friström B. Colour contrast sensitivity in ocular hypertension. A five-year prospective study. Acta Ophthalmol Scand. 2002;80(2):155-162.
- Richman J, Zangalli C, Lu L, Wizov SS, Spaeth E, Spaeth GL. The Spaeth/Richman contrast sensitivity test (SPARCS): design, reproducibility and ability to identify patients with glaucoma. Br J Ophthalmol. 2015;99(1):16-20.


