







Optical coherence tomography angiography (OCTA), adapted from traditional optical coherence tomography (OCT), is a robust noncontact, noninvasive imaging system that provides reproducible, 3-dimensional, high-resolution volumetric and quantitative data of the retinal layers including vascular networks in retina, optic nerve, and choroid. Its ability to show structural and vessel density information in both en face and depth-resolved imaging formats provides a better understanding of the glaucomatous process. My experience in OCTA is based on using the Optovue AngioVueHD system with AngioAnalytics software version 2018.0.0.18 (Optovue). This article will focus on describing and understanding the wide variety of information provided for each patient. Better understanding of the data and benefit to glaucoma patients of OCTA will encourage more ophthalmologists to incorporate this new technology into their practice.
Tables 1-4 show the OCTA results from patients in the Department of Ophthalmology at the University of Texas Southwestern Medical Center in Dallas, Texas: 74 normal healthy individuals, 26 glaucoma suspects, 34 patients with mild glaucoma, 27 with moderate glaucoma, and 9 with severe glaucoma.1 One of these patients is a 69-year-old female with well-controlled moderate glaucoma in the right eye and mild glaucoma in the left eye. Most of the scans refer to the right eye. The first step is to check for quality of the scan images, which is based on signal strength index (SSI), motion artifacts and blurriness of vascular features. A scan value of 6 or greater is preferable. The most common types of image artifacts should be excluded: motion (due to eye and lid movements), projection (images of blood vessels appear at false locations), retinal segmentation defects (false impressions of the density and locations of vessels), in addition to those caused by media opacities and corneal surface diseases.2
| RNFL Thickness (μm) | Healthy | Suspect | Mild | Moderate | Severe |
|---|---|---|---|---|---|
| Circumpapillary | 104.85±14 | 94.83±13.9 | 86.55±17.9 | 75.57±18.6 | 64.77±7.8 |
| Superior-hemi | 105±15.3 | 94.81±13.3 | 87.23±18.4 | 76.98±18.5 | 68.38±12.9 |
| Inferior-hemi | 104.69±14.7 | 94.84±16.5 | 85.81±18.7 | 74.05±20 | 60.9±7.8 |
| RNFL average thickness | 95.56±9.7 | 90.61±11.3 | 84.38±13 | 76.22±14.3 | 64.46±10.6 |
| RFNL; retinal nerve fiber layer. | |||||
| Ganglion Cell Complex | Healthy | Suspect | Mild | Moderate | Severe |
|---|---|---|---|---|---|
| Average thickness (μm) | 92.05±6.9 | 91.55±11 | 86.61±9.4 | 77.37±9.9 | 66.41±10.5 |
| Superior thickness (μm) | 91.71±6.6 | 93.23±14.9 | 87.13±8 | 78.2±10.4 | 67.44±11.9 |
| Inferior thickness (μm) | 92.41±7.7 | 89.89±9.3 | 86.1±11.3 | 76.55±10.7 | 65.44±9.7 |
| Focal loss volume (%) | 1.09±1.8 | 2.09±2.3 | 2.63±3.7 | 5.59±3.5 | 9.02±5.3 |
| Global loss volume (%) | 5.07±4.9 | 7.57±5.1 | 9.76±8.4 | 18.21±9.1 | 29.41±10.5 |
| Optic Nerve Head Vessel Density (%) | Normal | Suspect | Mild | Moderate | Severe |
|---|---|---|---|---|---|
| Whole image | 48.09±3.5 | 45.49±4.7 | 43.29±5.9 | 38.64±7.1 | 32.44±3.7 |
| Inside disc | 47.31±6.5 | 48.22±5 | 46.67±7.2 | 42.38±7.7 | 41.07±11 |
| Circumpapillary | 50.74±4.5 | 47.11±5.7 | 45.09±7.9 | 40.27±8.4 | 31.49±4.1 |
| Superior hemifield | 51.17±4.7 | 47.7±6.1 | 45.67±7.7 | 41.25±8.7 | 31.78±4.6 |
| Inferior hemifield | 50.27±4.5 | 46.47±5.5 | 44.45±8.6 | 39.21±8.6 | 31.16±5 |
| Retinal Vessel Density (%) | Normal | Suspect | Mild | Moderate | Severe |
|---|---|---|---|---|---|
| Central | 15.54±5.7 | 15.01±6.3 | 14.84±7.2 | 15.77±6.3 | 12.29±5.9 |
| Temporal | 45.3±4.3 | 43.68±7.4 | 43.06±6.4 | 39.46±6.1 | 31.18±5.6 |
| Superior | 48.1±5.1 | 47.07±6.3 | 45.98±5.6 | 42.83±5.6 | 35.62±4.7 |
| Nasal | 46.4±5.1 | 46.22±5.8 | 44.47±5.7 | 41.59±6.5 | 35.01±4.6 |
| Inferior | 47.59±4.3 | 45.54±6.9 | 44.22±6.7 | 41.65±7 | 33.81±4.3 |
Figure 1 summarizes several variables, including retinal nerve fiber (RNFL): average, superior, inferior, and intraeye differences. Similarly, ganglion cell complex (GCC) values include average, superior, and inferior; intraeye; focal loss volume percentage (FLV%); and global loss volume percentage (GLV%). Focal loss volume indicates areas of focal defects in the GCC topography, whereas GLV represents generalized thinning of GCC layers. The optic nerve head (ONH) analysis table provides information on the cup-to-disc area ratio, rim area, disc area, and cup volume. Measurements of RNFL thickness are shown in a TSNIT orientation and are compared to age-matched controlled individuals. The green area denotes the fifth to ninety-fifth percentile by age, the yellow area is the first to fifth percentile, and the red area is below the first percentile. Tables 1 and 2 show the results derived from our patient population.
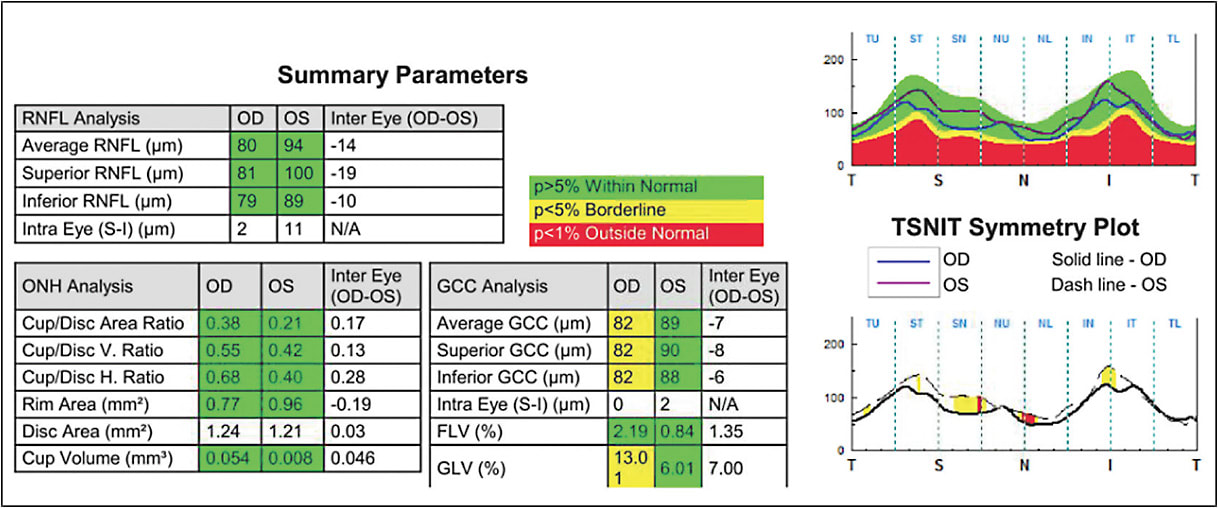
Figure 2 focuses on optic nerve parameters, including RNFL thickness and radial peripapillary capillary (RPC) density percentage. The preferred term is circumpapillary vessel density percentage. The RNFL thickness (internal limiting membrane-NFL) map is based on the Garway-Heath grid areas.3 Cool colors are areas of decreased thickness, whereas warm colors are areas of increased thickness. Thickness values are populated within the grid. The structural parameters are shown in the ONH analysis table supported by RNFL thickness, hemifield, and 4-quadrant RNFL thickness. AngioAnalytics software vessel density mapping computes the percentage of area occupied by OCTA-detected vasculature based on the circumpapillary capillary slab in the Garway-Heath grid areas. Cool colors show areas of lower density while warm colors show areas of greater density. Vessel density parameters are populated in the grid. Global and capillary RPC vessel density parameters are shown in the small vessels box. Separately, in the middle are numbers from the hemifield and 4 quadrant areas (Table 3).
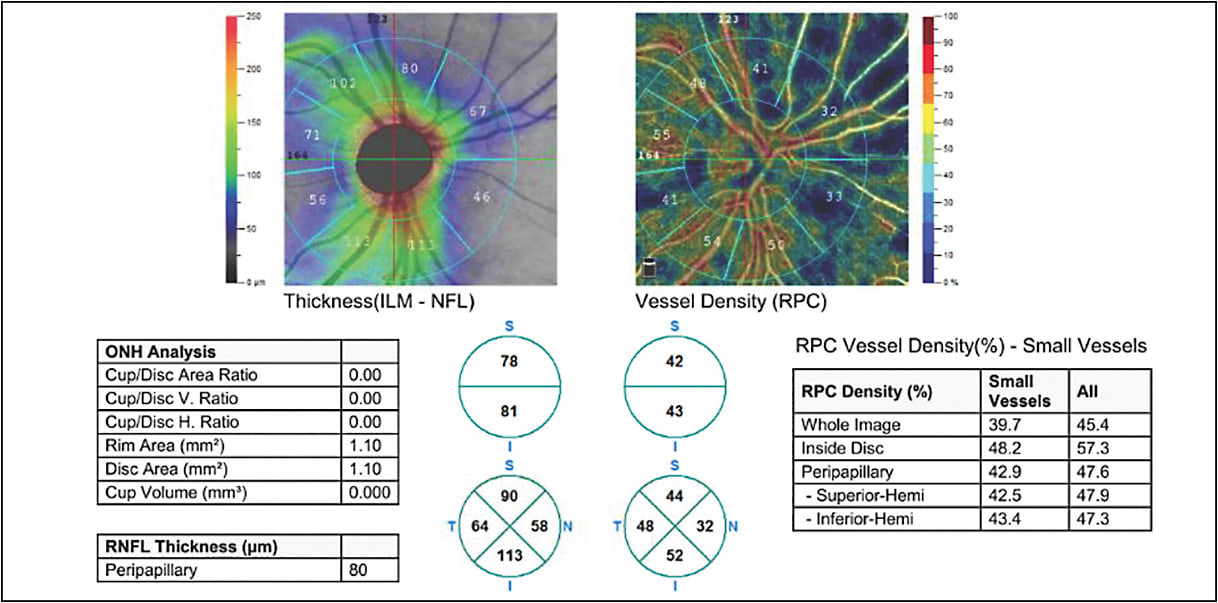
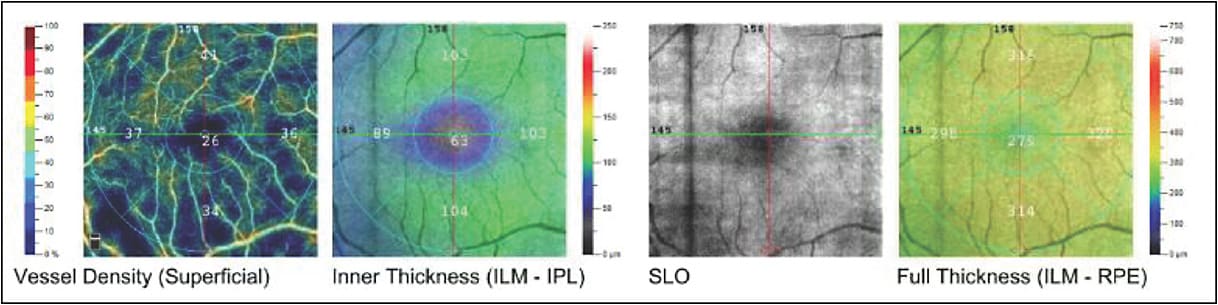
Figure 3 relates to retinal vasculature and thickness (angio retina quickVue) scan. AngioAnalytics vessel density mapping computes the percentage of area occupied by OCTA-detected vessels based on both the superficial and deep vasculature complexes. Cool colors are areas of lower density, whereas warm colors are areas of greater density. Vessel density parameters are populated within the ETDRS grid.4 The retinal thickness map of the inner retina (internal limiting membrane to inner plexiform layer) with ETDRS overlay shows areas of decreased thickness in cool colors and areas of increased thickness in warm colors. There is a scanning laser ophthalmoscopy (SLO)-like image of the retina as well. Lastly, a full retinal thickness map (internal limiting membrane to retinal pigment epithelium) with ETDRS grid overlay shows cool colors as areas of decreased thickness and warm colors as areas of increased thickness. Thickness parameters are also populated within the ETDRS grid (Table 4).
Optical coherence tomography angiography also demonstrates foveal avascular zone (FAZ) metrics based on full retinal vasculature (internal limiting membrane to outer plexiform layer +10 µm). In addition, the acircularity index (ratio between the measured perimeter of the same size circular area) is available. Acircularity index is correlated with advancing retinal disease process and vessel density within a 300 µm width ring surrounding the FAZ. The other scans are an SLO-like en face (looking at the face of retina) image and a horizontal B-scan of the retina.
Future of OCTA
The scope of OCTA has widened to encompass management of other systemic diseases, such as Alzheimer disease, multiple sclerosis, anterior ischemic optic neuropathy, and Leber hereditary optic neuropathy.5 Researchers have shown that patients with Alzheimer disease exhibit a reduced flow density in the radial circumpapillary capillary layer and in the superficial retinal layers when compared with healthy controls.6 In addition, FAZ was found to be enlarged in patients with preclinical Alzheimer disease.7
Adaptive optics (AO) technology is often used to correct wavefront distortions or aberrations as light travels through complex optical systems such as the eye. This enhances image resolution and facilitates diffraction-limited optics, which has been used to visualize key retinal structures in the eye.8 Optical coherence tomography provides images at the tissue level in the axial dimension, but its transverse resolution is limited by ocular aberrations. It cannot be used for imaging at the cellular level without the aid of AO. Combining these would provide 3-dimensional imaging, at near-video rates, of the microscopic retinal cellular structures and may help clinical diagnosis and research of the eye.9 Recent work by Liu et al using AO-OCT has demonstrated somas of ganglion cells including their 3-dimensional mosaic pattern, primary subtypes, and spatial projection to other neurons that may be critical in early diagnosis of glaucoma and other neuronal diseases.10
Swept-source OCT has also been explored for overcoming high-speed imaging failings. The longer wavelength of 1,050 nm used by swept-source OCT is considered ideal for deeper structures such as the choroid and optic nerve head. Currently both swept-source and AO technologies are expensive, but these technologies have promise for the future of retinal imaging. GP
References
- Yang A, Noorani S. Deng T, Al Salem M, Adams-Huet B, Li X, Kooner K. Power of OCT-A (Optical Coherence Tomography Angiography) in glaucoma. Presented at the Annual Meeting of the American Glaucoma Society in New York, New York, March 1-4, 2018.
- Spaide, RF, Fujimoto, Waheed NK. Image artifacts in optical coherence angiography. Retina. 2015;35(11):2163-2180.
- Garway-Heath DF, Hitchings RA. Quantitative evaluation of the optic nerve head in early glaucoma. Br J Ophthalmol. 1998;82(4):352-361.
- Early Treatment Diabetic Retinopathy Study Research Group. Early treatment diabetic retinopathy study design and baseline patient characteristics: ETDRS Report Number 7. Ophthalmology. 1991;98(5):741-756.
- Wang L, Olwen M, Natalia GC, Calabresi PA, Saidha S. Emerging applications of optical coherence tomography angiography in neurological research. Eye Vis (Lond). 2018;5:11.
- Lahme L, Esser EL, Mihailovic N, et al. Evolution of ocular perfusion in Alzheimer’s disease using optical coherence tomography angiography. J Alzheimers Dis. 2018;66(4):1745-1752.
- O’Bryhim BE, Apte RS, Kung N, Coble D, Van Stavern GP. Association of preclinical Alzheimer disease with optical coherence tomography angiography findings. JAMA Ophthalmol. 2018;136(11):1242-1248.
- Liang J, Williams DR, Mill DT. Supernormal vision and high-resolution retinal imaging through adaptive optics. J Opt Soc Am A Opt Image Sci Vis. 1997;14(11):2884-2892.
- Liu Z, Tam J, Saeedi O, Hammer DX. Trans-retinal cellular imaging with multimodal adaptive optics. Biomed Opt Express. 2018;9(9):4246-4262.
- Liu Z, Kurokawa K, Zhang F, Lee JJ, Miller DT. Imaging and quantifying ganglion cells and other transparent neurons in the living human retina. Proc Nat Acad Sci. 2017;114(48):12803-12808.
