







Patients are asking a lot about US healthcare macroeconomics. However, they tend to phrase the questions in simpler formats when talking to their physicians. For example, they might ask, “Why do I have to wait so long for an appointment?” or, “Why is your office so busy?”
In March of 2018, the Association of American Medical Colleges (AAMC) released their update on physician supply and demand.1 This report analyzes the factors driving demand and supply of physicians. It considers the changing demographics of the American population, different insurance and provider models, trends in the physician workforce, and a host of other factors.
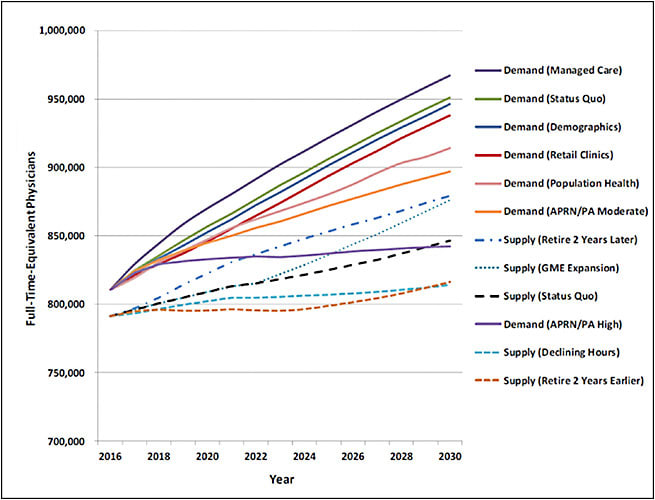
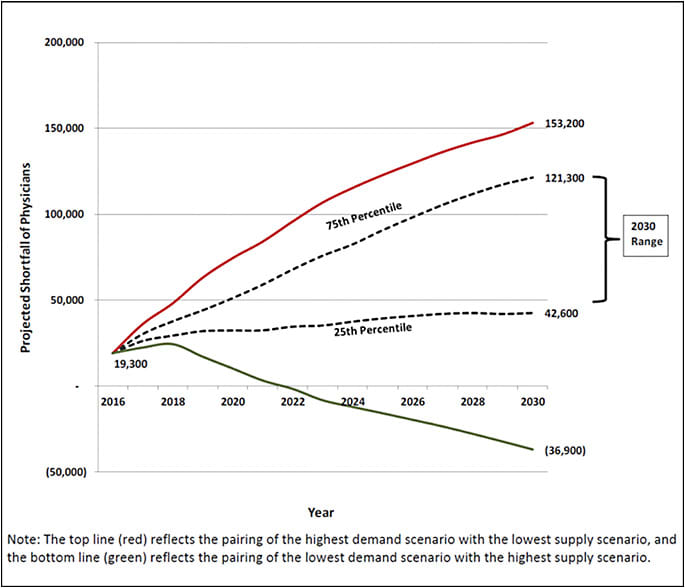
The report from the AAMC forecasts worsening physician shortages in primary care and subspecialties between now and 2030 (the end of the analysis). The summary predicts that physician demand will grow faster than supply, leading to a projected total shortfall of between 42,600 and 121,300 physicians, including a shortfall of between 14,800 and 49,300 primary care physicians and between 33,800 and 72,700 specialists.
The increased projected shortfalls are driven by several factors. On the demand side, the US population is expected to grow about 11% with a 50% increase in the population over age 65, which has a higher per capita demand for health care. Of course, older populations have a higher prevalence of glaucoma as well. Success in health management leading to longer lives and success in expanding access to underserved populations add to the shortfalls.
On the supply side, earlier physician retirement may worsen supply, especially because 40% of active physicians are age 55 or greater. The trend of physicians working fewer hours per week may account for the equivalent of 32,500 fewer full-time-equivalent physicians by 2030. Scenarios with greater employment of nurse practitioners and physician assistants may mitigate these trends somewhat.
Put simply, physicians are, on average, busy, and likely to become more so. Wait times to schedule appointments are likely to lengthen. The demands on physicians to see greater numbers of patients will increase, exacerbating busy waiting rooms and potentially straining professional standards.
How can we communicate this effectively and succinctly to patients, while maintaining a positive outlook? First, patients tend to easily grasp that our population is growing, and they understand that an aging population requires more health care. Patients are willing to accept, but have often not considered, that there is a finite number of medical schools, and that although more are opening, it is a slow process and it takes a long time for a new student to become a fully trained physician.
It is more of a challenge for patients to consider that physicians cannot simply work more hours, and that seeing fewer patients in a day might mean that they themselves might be the ones not seen. I find this discussion least productive when a patient is already frustrated by a long wait.
It’s incumbent upon all physicians to look for ways to maximize the benefit we can provide our patients. For glaucoma specialists and general ophthalmologists treating glaucoma, the solution to creating efficiency depends greatly on practice patterns, patient population, and other factors specific to each physician. Electronic health records, limited technicians, meaningless exam requirements, prior authorizations, and other hurdles stand in our way, but physicians are in the best position to optimize care delivery. Also, we are most likely to prefer our solutions to those chosen for us by others. GP
Reference
- Dall T, West T, Chakrabarti R, Reynolds R, Iacobucci W. 2018 update: the complexities of physician supply and demand: projections from 2016 to 2030. Association of American Medical Colleges. 2018; Association of American Medical Colleges and IHS Markit Ltd. Available at https://aamc-black.global.ssl.fastly.net/production/media/filer_public/85/d7/85d7b689-f417-4ef0-97fb-ecc129836829/aamc_2018_workforce_projections_update_april_11_2018.pdf
