







Glaucoma specialists in the United States spend a great deal of time managing open-angle disease, which accounts for the great majority of glaucoma cases. The treatment paradigms for these cases are particularly ingrained in their minds. Less ingrained is the treatment paradigm for patients on the “angle closure spectrum” who have closed or narrow angles.
Treatment options exist for every stage of angle closure, and this enables glaucoma specialists to make choices based on the treatment goals, risks, age, other eye conditions, and previous surgeries. The data and information available on the nature of the angle closure spectrum, how to prevent progression, and how glaucomatous damage can occur show that a pragmatic stepwise approach works best.1-4
Classifying Angle-closure Pathology
Among the 3 stages of angle closure — primary angle closure suspect (PACS), primary angle closure (PAC), and primary angle closure glaucoma (PACG) — PACS is by far the most common.5,6 Very few patients with PACS will develop the trabecular damage that characterizes PAC, and fewer still progress to the measurable optic neuropathy that indicates PACG.7
Although there are numerous systems to classify the angle anatomy and configuration, among the simplest is to describe the angle structures seen using dynamic gonioscopy. For example, if only Schwalbe’s line is visible, then the angle is either closed (PAC) or in apposition (PACS). If some or all of the trabecular meshwork is visible, then the patient may have a narrow angle (PACS) or an open angle.
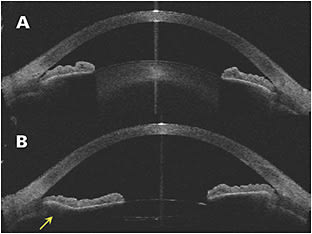
Dynamic gonioscopy allows practitioners to see structures more clearly and make the diagnosis. For example, the appositional angles of PACS deepen with dynamic gonioscopy, whereas closed angles do not deepen. Baseline measurements of the angles are obtained, which allow for grading of angle closure. Anterior-segment optical coherence tomography (OCT) or ultrasound biomicroscopy can provide further clarification if the anatomy is uncertain.8 In the author’s experience, anterior-segment OCT is also a helpful tool for explaining to skeptical patients with asymptomatic PACS or PAC that they do have a problem that requires treatment (Figure 1).
Treatments and Monitoring
A patient with PACS is at risk of having an angle closure crisis (ACC). Traditionally, iridotomy has been performed to prevent ACC.9,10 In the recent Zhongshan Angle-Closure Prevention (ZAP) trial, iridotomy provided a moderate effect.11 It prevented patients from reaching a sight-threatening crisis, but because such crises are not common, the study recommended against routine iridotomy for PACS. This conclusion has caused some debate and led physicians to define PACS iridotomy candidates more narrowly.12 Iridotomy is still an option for PACS patients with appositional angles greater than 180° to prevent ACC, although it may not prevent conversion from PACS to PAC (defined by anatomic or functional evidence of trabecular damage).
Although iridotomy limits or eliminates their risk of an ACC episode, patients can still develop peripheral anterior synechiae (PAS) between the peripheral iris and the trabecular meshwork or peripheral cornea as their crystalline lens matures and enlarges, so they must be followed over the years.
PACS patients should be followed over time, with the surgeon performing gonioscopy to check their angles. If adhesions form, or there is a consistent increase in intraocular pressure (IOP) after iridotomy, then the patient has developed trabecular dysfunction and converted from PACS to PAC. By advancing along the spectrum, these patients now face a higher risk of developing optic neuropathy with PACG.13
With PAC, iridotomy remains an option to provide some trabecular recovery. For patients in their mid-50s or older who have already had an iridotomy, cataract surgery (phacoemulsification) is often recommended. This practice is supported by the results of the EAGLE study,14 which demonstrated the effectiveness of lens extraction in treating patients with PAC and PACG. Clear lens extraction poses an increased risk of retinal tears in younger patients, even after uncomplicated phacoemulsification,15 so peripheral iridoplasty is preferred.
Determining the Best Treatment for PACG
For patients with PACG, defined as angle closure combined with measurable glaucoma damage, cataract surgery combined with a glaucoma procedure is recommended. Goniosynechialysis is an option if anterior synechiae are present. If the patient has mild or moderate glaucoma damage and/or elevated IOP, then endocyclophotocoagulation (ECP) (BVI Endo Optiks E2 laser and endoscopy system) at the time of the cataract surgery is effective.16-19
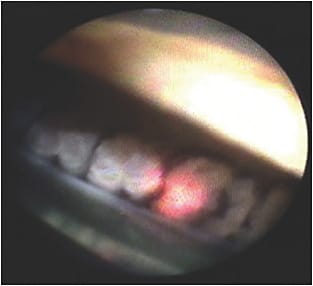
Endocyclophotocoagulation has 2 beneficial effects: (1) it ablates the ciliary epithelium and can decrease aqueous production, thereby decreasing IOP; and (2) it shrinks the ciliary processes, causing the peripheral iris to rotate posteriorly and mechanically open the anterior-chamber angle (termed endocycloplasty) (Figure 2).20-23
During the procedure, the anterior chamber is filled with dispersive viscoelastic prior to phacoemulsification, and 360° intraoperative gonioscopy is performed. If the PAS noted in the clinic peel back with this maneuver alone, then repeat gonioscopy is not necessary after phaco, but if there are areas of PAS and angle closure, particularly more than 1 clock hour, then gonioscopy is required after ECP.
Routine phacoemulsification is performed next, followed by implantation of the intraocular lens and evacuation of the cohesive viscoelastic from the capsular bag. An adaptive viscoelastic agent (Healon GV, Johnson & Johnson; or Amvisc Plus, Bausch + Lomb) widens the ciliary sulcus space, and the surgeon performs 360° ECP using a 19-gauge curved laser microendoscope. This procedure requires a second 2-mm to 2.5-mm keratome incision nasally. After ECP, viscoelastic is removed from the ciliary sulcus, and the anterior chamber is reformed with the same adaptive viscoelastic, with the surgeon taking care to widen the angle with the ophthalmic viscosurgical device. The surgeon does a final check to see whether goniosynechiae are still present or whether they have lysed themselves through the surgical forces and posterior rotation of the ciliary processes and peripheral iris. If synechiae are still present, then goniosynechialysis is performed.
The approach is different when a patient presents with PACG, having already developed moderate or severe glaucoma damage. In these cases, phaco/ECP with goniosynechialysis can open the angle, but that may not be enough on its own, and the patient may have a pressure spike in the immediate postoperative period or poor IOP control. An additional filtering surgery can be added, such as trabeculectomy, tube shunt, or Xen gel stent (Allergan).
Glaucoma Progression After Surgical PACG Treatment
When glaucomatous changes occur after treatment for PACG, it is often described as secondary open-angle glaucoma, although the mechanism of trabecular damage is unchanged. Like other patients with open-angle glaucoma, these patients can be controlled with medication or surgical intervention. With the angle opened, they may be candidates for angle-based procedures or traditional filtering surgeries and tube shunts.
The choice of surgical intervention depends on the staging of glaucoma. Options include standalone nonstenting procedures, like the Kahook Dual Blade (New World Medical), trabectomy, the OMNI Glaucoma Treatment System (Sight Sciences), and ab interno canaloplasty (ABiC; Ellex). These procedures are effective in lowering pressure and minimizing optic nerve damage in mild- to moderate-stage glaucoma. Like all other stages of the angle-closure spectrum, treatment choices for glaucoma after PACG therapy should generally follow a stepwise approach, with more aggressive filtering interventions considered for more severe stages of the disease. GP

References
- Ng WT, Morgan W. Mechanisms and treatment of primary angle closure: a review. Clin Exp Ophthalmol. 2012;40(4):e218-e228. doi:10.1111/j.1442-9071.2011.02604.x
- Thomas R, Walland MJ. Management algorithms for primary angle closure disease. Clin Exp Ophthalmol. 2013;41(3):282-292. doi:10.1111/ceo.12209
- Lai J, Choy BNK, Shum JWH. Management of primary angle-closure glaucoma. Asia Pac J Ophthalmol (Phila). 2016;5(1):59-62. doi:10.1097/APO.0000000000000180
- Chan PP, Pang JC, Tham CC. Acute primary angle closure-treatment strategies, evidences and economical considerations. Eye (Lond). 2019;33(1):110-119. doi:10.1038/s41433-018-0278-x
- Moghimi S, Torkashvand A, Mohammadi M, et al. Classification of primary angle closure spectrum with hierarchical cluster analysis. PLoS One. 2018;13(7):e0199157. doi:10.1371/journal.pone.0199157
- Kim YK, Choi HJ, Jeoung JW, Park KH, Kim DM. Five-year incidence of primary open-angle glaucoma and rate of progression in health center-based Korean population: the Gangnam eye study. PLoS One. 2014;9(12):e114058. doi:10.1371/journal.pone.0114058
- Thomas R, George R, Parikh R, Muliyil J, Jacob A. Five year risk of progression of primary angle closure suspects to primary angle closure: a population based study. Br J Ophthalmol. 2003;87(4):450-454. doi:10.1136/bjo.87.4.450
- Chansangpetch S, Rojanapongpun P, Lin SC. Anterior segment imaging for angle closure. Am J Ophthalmol. 2018;188:xvi-xxix. doi:10.1016/j.ajo.2018.01.006
- Wright C, Tawfik MA, Waisbourd M, Katz LJ. Primary angle-closure glaucoma: an update. Acta Ophthalmol. 2016;94(3):217-225. doi:10.1111/aos.12784
- Radhakrishnan S, Chen PP, Junk AK, Nouri-Mahdavi K, Chen TC. Laser peripheral iridotomy in primary angle closure: a report by the American Academy of Ophthalmology. Ophthalmology. 2018;125(7):1110-1120. doi:10.1016/j.ophtha.2018.01.015
- He M, Jiang Y, Huang S, et al. Laser peripheral iridotomy for the prevention of angle closure: a single-centre, randomised controlled trial. Lancet. 2019;393(10181):1609-1618. doi: 10.1016/S0140-6736(18)32607-2
- Gupta V, Dada T. Should we perform peripheral laser iridotomy in primary angle closure suspects: implications of the ZAP trial? Ann Transl Med. 2019;7(Suppl 3):S157. doi:10.21037/atm.2019.06.52
- Thomas R, Parikh R, Muliyil J, Kumar RS. Five-year risk of progression of primary angle closure to primary angle closure glaucoma: a population-based study. Acta Ophthalmol Scand. 2003;81(5):480-485. doi:10.1034/j.1600-0420.2003.00135.x
- Azuara-Blanco A, Burr J, Ramsay C, et al. Effectiveness of early lens extraction for the treatment of primary angle-closure glaucoma (EAGLE): a randomised controlled trial. Lancet. 2016;388(10052):1389-1397. doi:10.1016/S0140-6736(16)30956-4
- Erie JC, Baratz KH, Mahr MA, Johnson DH. Phacoemulsification in patients with Baerveldt tube shunts. Cataract Refract Surg. 2006;32(9):1489-1491. doi:10.1016/j.jcrs.2006.04.008
- Panse K, Le C, Hubbell M, Ayyala RS. Surgical outcomes of phacoemulsification/goniosynechialysis with and without endocyclophotocoagulation in patients with chronic angle closure glaucoma. Indian J Ophthalmol. 2019;67(3):366-370. doi:10.4103/ijo.IJO_895_18
- Francis BA, Pouw A, Jenkins D, et al. Endoscopic cycloplasty (ECPL) and lens extraction in the treatment of severe plateau iris syndrome. J Glaucoma. 2016;25(3):e128-e133. doi:10.1097/IJG.0000000000000156
- Pathak-Ray V. Intermediate results of phaco-endocycloplasty in an exclusive cohort of angle closure glaucoma: potential for change. Int Ophthalmol. 2019;39(10):2257-2265. doi:10.1007/s10792-018-01062-9
- Hollander DA, Pennesi ME, Alvarado JA. Management of plateau iris syndrome with cataract extraction and endoscopic cyclophotocoagulation. Exp Eye Res. 2017;158:190-194. doi:10.1016/j.exer.2016.07.018
- Zhou WS, Lin WX, Geng YY, Wang T. Combined phacoemulsification and goniosynechialysis with or without endoscopic cyclophotocoagulation in the treatment of PACG with cataract. Int J Ophthalmol. 2020;13(9):1385-1390.
- Perez Bartolome F, Rodrigues IA, Goyal S, et.al. Phacoemulsification plus endoscopic cyclophotocoagulation versus phacoemulsification alone in primary open-angle glaucoma. Eur J Ophthalmol. 2018;28(2):168-174. doi:10.5301/ejo.5001034
- Cohen A, Wong SH, Patel S, Tsai JC. Endoscopic cyclophotocoagulation for the treatment of glaucoma. Surv Ophthalmol. 2017;62(3):357-365. doi:10.1016/j.survophthal.2016.09.004
- Rodrigues IAS, Lindfield D, Stanford MR, Goyal S. Glaucoma surgery in scleromalacia: using endoscopic cyclophotocoagulation where conventional filtration surgery or angle procedures are contraindicated. J Curr Glaucoma Pract. 2017;11(2):73-75. doi:10.5005/jp-journals-10028-1227