







In May 2024, 5 Medicare Administrative Contractors (MACs) published proposed local coverage determinations (LCDs) for microinvasive glaucoma surgery (MIGS). They subsequently held public hearings in June. While the 2023 proposed LCDs on this topic caused a sensation in the ophthalmic community and elicited strong criticism, the mid-year public hearings were a model of decorum, with few objections from professional societies, surgeons, or industry.1
On October 3, 2024, Noridian published a final LCD version with an effective date of November 17, 2024; other MACs will follow suit soon. The final LCD is largely unchanged from the proposed LCD. Noridian made no coverage changes based on new literature submitted during the comment period and reaffirmed a policy of coverage for cataract and a single MIGS procedure. It states, “combining multiple [MIGS] procedures on the same eye in the same day is non-covered.”2
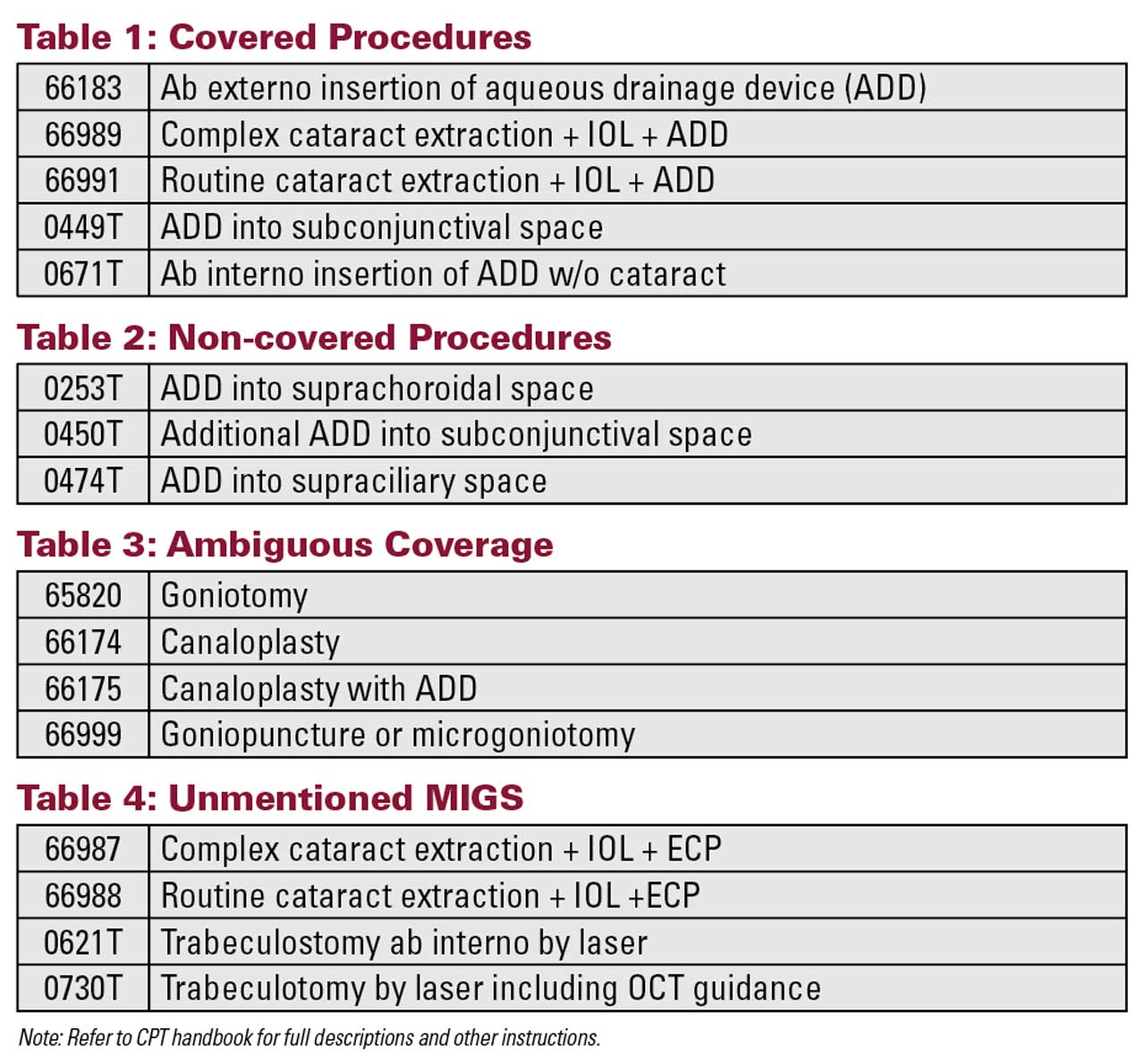
The 11,000-word LCD and companion article provide explicit guidance on covered and non-covered procedures but is ambiguous or silent on some related topics mentioned previously (Table 1-4). The LCD also establishes critical limitations of coverage:
- MIGS is not a first-line treatment for mild to moderate glaucoma (in lieu of medical management);
- Combined aqueous shunt and MIGS cannot be performed at the same time in the same eye;
- Xen gel stent (AbbVie) insertion must be performed by an ophthalmologist experienced in trabeculectomy and bleb management;
- The number of stents allowed will be consistent with the stents contained within the device;
- Multiple stents (so-called “dosing”), regardless of method, is not supported by sufficient evidence;
- One iStent infinite (Glaukos) per eye for refractory glaucoma; and
- One Xen gel stent per eye for refractory glaucoma.
In the pivotal trial for the Xen gel stent, refractory glaucoma was defined as “prior failure of a filtering/cilioablative procedure OR uncontrolled intraocular pressure (IOP) defined as progressive damage or mean diurnal medicated IOP ≥20 mmHg on maximally tolerated medical therapy (ie, ≥4 classes of topical IOP-lowering medications, or fewer in the case of tolerability or efficacy issues).”3 (In the September 2024 issue of Glaucoma Physician, I discussed the definition of refractory glaucoma in detail.4)
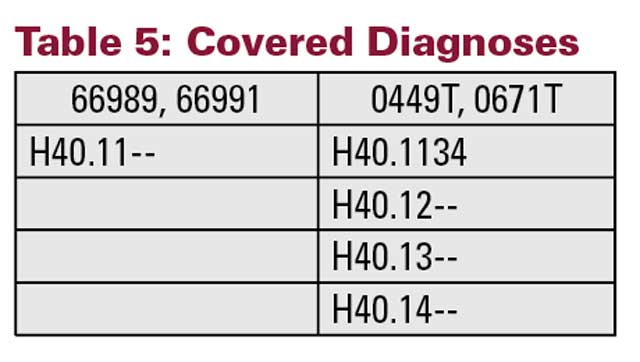
The associated article with the LCD provides a defined list of covered diagnoses that also limit coverage (Table 5).5
Where cataract surgery is performed at the same time as a MIGS procedure and in the same eye, the Medicare coverage criteria for cataract must also be satisfied. Otherwise, the entire claim is at risk of being denied.
This new LCD is in response to a rapid increase in MIGS procedures from 2013 to the present, with the Intelligent Research in Sight (IRIS) Registry expressing concern about the relative expense and unknown long-term safety and efficacy of these procedures. The medical directors at these MACs share that concern. According to the LCD, the authors of the American Academy of Ophthalmology’s preferred practice pattern for glaucoma “acknowledge lack of evidence for several of the MIGS techniques.”6 In this context, it is anticipated that MACs will make more requests for additional documentation prior to processing claims for reimbursement of MIGS. Essential documentation in the surgeon’s medical records should include:
- Anti-glaucoma medication(s) success/failure;
- Compliance with medications;
- Filtration/cilioablation procedure(s) if performed;
- Gonioscopy;
- Laser trabeculoplasty if
performed; - Longitudinal IOP;
- Operative report with patient-specific indication(s);
- Optic nerve imaging showing abnormalities;
- Perimetry that establishes
glaucoma stage; and - Target IOP.
Importantly, where the risks, benefits, and alternatives of MIGS are discussed with the patient, the surgeon should also explain what is covered and what is not. Where coverage is uncertain, financial waivers should be required prior to surgery for the surgeon and the facility. An LCD does not restrict what the surgeon can do, it just describes what Medicare will or will not pay for. GP

References
1. Centers for Medicare and Medicaid Services. Noridian A59897 response to comments: micro-invasive glaucoma surgery (MIGS). September 17, 2024. Accessed October 7, 2024. https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleId=59897
2. Centers for Medicare and Medicaid Services. Noridian LCD L38301 micro-invasive glaucoma surgery (MIGS). October 3, 2024. Accessed October 7, 2024. https://www.cms.gov/medicare-coverage-database/view/lcd.aspx?lcdid=38301
3. Sheybani A, Vera V, Grover DS, et al. Gel stent versus trabeculectomy: the randomized, multicenter, gold-standard pathway study (GPS) of effectiveness and safety at 12 months. Am J Ophthalmol. 2023;252:306-325. doi:10.1016/j.ajo.2023.03.026
4. Corcoran, KJ. Defining Refractory Glaucoma. Glaucoma Physician. September 1, 2024. Accessed October 7, 2024. https://digital.glaucomaphysician.net/articles/defining-refractory-glaucoma
5. Centers for Medicare and Medicaid Services. Noridian A57864 billing and coding: micro-invasive glaucoma surgery (MIGS). September 17, 2024. Accessed October 7, 2024. https://www.cms.gov/medicare-coverage-database/view/article.aspx?articleId=57864
6. Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern. Ophthalmology. 2021;128(1):71-150. doi:10.1016/j.ophtha.2020.10.022