







Traditionally, the surgical space for cataract surgery has been very limited for primary open-angle glaucoma (POAG) patients. Fortunately, today we are on the forefront of innovation when it comes to finding a solution for these patients, because there are multiple lens implant choices that can help us push limits and provide satisfying visual outcomes.
As per the American Society of Cataract and Refractive Surgery (ASCRS) subcommittee on glaucoma, every glaucoma patient is entitled to choices for presbyopia-mitigating intraocular lens (IOL) implants, provided they are a candidate.1 Therefore, it is our commitment as surgeons to explore these potential choices for our patients.
Clinical considerations include the degree of ocular surface disease related to chronic drop therapy, as well as the amount of optic nerve damage due to glaucoma. If the patient has a mild case or is considered a suspect with no retinal nerve fiber layer (RNFL) loss or visual field deficits, a traditional diffractive multifocal lens can still be considered for presbyopia correction. With more tissue loss or small peripheral defects, an extended depth of focus (EDOF) lens like the Tecnis Symfony OptiBlue (Johnson & Johnson Vision) or the Clareon Vivity nondiffractive lens (Alcon) can be considered. And with mild to moderate glaucoma with more involvement, the Light Adjustable Lens+ (LAL+; RxSight) can be considered.
Address Problems With the Ocular Surface First
Research has found that 50% to 90% of glaucoma patients suffer from some form of ocular surface disease (OSD).2 If we wish to achieve consistent surgical results, we must prioritize fixing the ocular surface prior to biometry. When meibomian gland dysfunction (MGD) is noted, treatments such as thermal pulsation and intense pulsed light (IPL) can be employed to improve the tear film.
If there is significant corneal staining, regenerative tools such as amniotic membrane or cyclosporine/serum tears can be employed. Recently, we employed Prokera Slim (BioTissue) cryopreserved amniotic membrane in a 79-year-old female patient with longstanding moderate glaucoma. Her chronic use of ophthalmic brimonidine drops and Vyzulta (Bausch + Lomb) contributed to punctate keratitis, which improved dramatically with placement of Prokera on each eye for 3 days at a time (Figure 1).
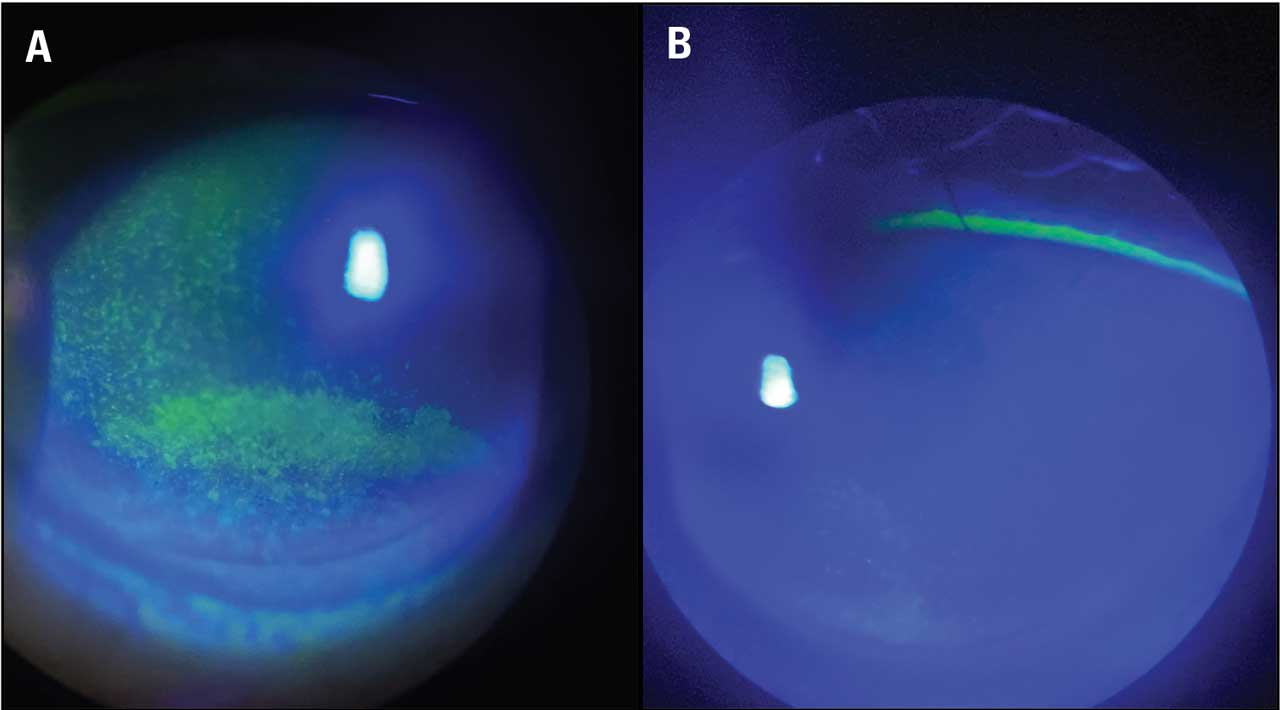
Figure 1. Corneal staining (A) in a 79-year-old patient preparing for cataract surgery. The ocular surface was greatly improved (B) after amniotic membrane therapy. Images courtesy Zarmeena Vendal, MD.
In 2022, we published a case series of glaucoma patients who received amniotic membrane to help heal their OSD.3 These patients not only showed improvement in corneal staining due to their chronic topical medication therapy, but also gained 1 to 3 lines improvement in visual acuity. This level of improvement can make a valuable difference in obtaining a higher quality of biometry in preparation for surgery.
Diffractive IOLs
It is important to note that traditional diffractive multifocal IOL implants are still an option for patients who are glaucoma suspects or have mild POAG but have preserved RNFL and perimetry. We recently treated a physician patient who was interested in reducing her spectacle dependence but was a POAG suspect due to a family history of glaucoma and her elevated IOP. We implanted the Clareon PanOptix trifocal lens (Alcon), the only FDA-approved trifocal currently available in the United States. The patient achieved 20/20 J1 vison. More importantly, she was able to perform her clinical duties daily without the need for reading glasses, which made a significant addition to her quality of life.
EDOF Lenses
Extended depth of focus lenses can also be employed successfully for the glaucoma patient. The Vivity IOL is a nondiffractive EDOF lens implant that can safely be used in patients who do exhibit RNFL loss and even mild peripheral VF defects. Patients can achieve 20/20 J2 vision with no nighttime halo effect when this implant is used in mini-monovision fashion, with a -.50 D target in the nondominant eye.
The Symfony OptiBlue lens warrants discussion due to its multifocal and EDOF properties. Mini-monovision targets with this lens implant result in similar 20/20 J2 results, but with reduced glare and halo at night. At the ASCRS April 2024 annual meeting in Boston, we presented a case series of glaucoma suspect and mild POAG patients who achieved consistent visual results at 6 months (Figure 2). All have reported (on standard questionnaire) that they would pick the OptiBlue lens again.4
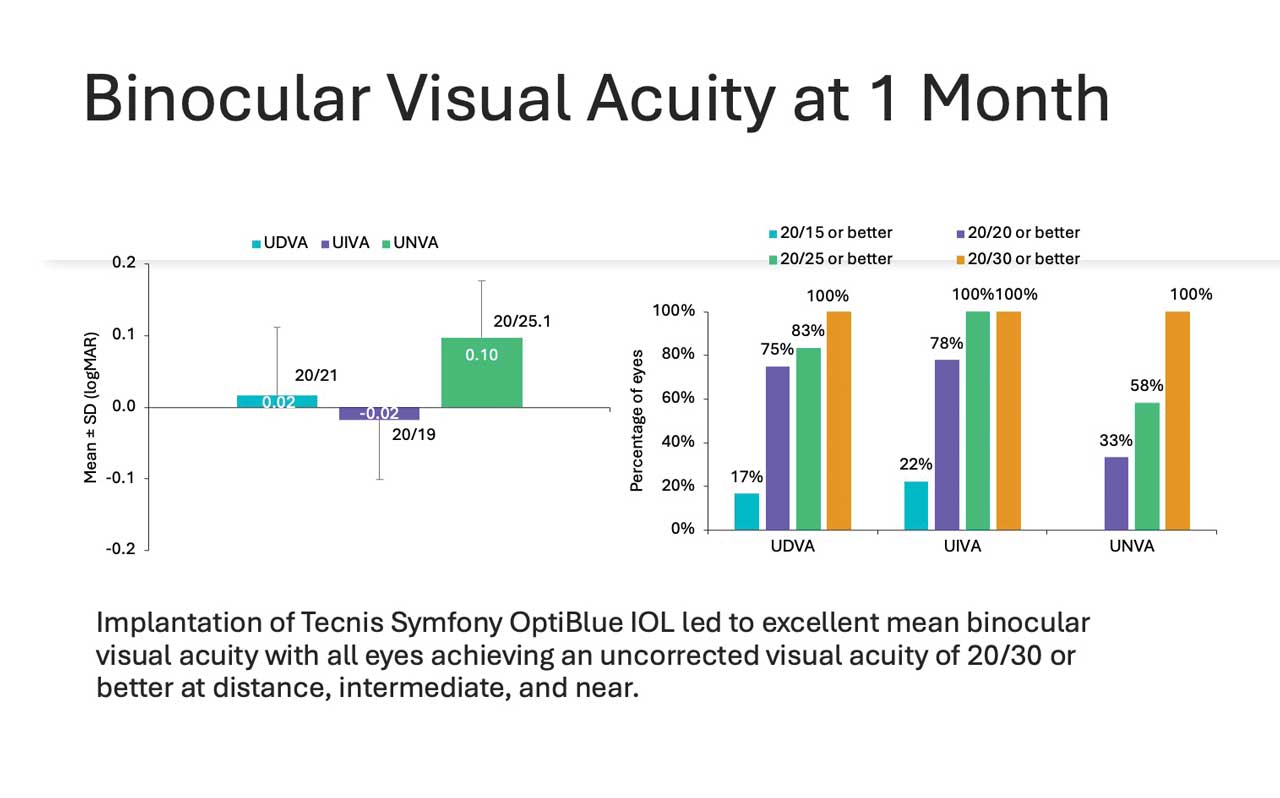
Figure 2. According to a case series presented at the 2024 ASCRS meeting, 100% of eyes implanted with the Symfony OptiBlue intraocular lens achieved an uncorrected visual acuity of 20/30 or better at distance, intermediate, and near.
Finally, with more significant visual field defects, monovision is still a viable option for presbyopia mitigation in glaucoma patients. The LAL+ lens is unique in its properties to customize near targeting, which can be especially helpful in reducing depth perception issues in the glaucoma patient. There are no nighttime aberration concerns given this is a monofocal platform, and patients can really participate in the setting of their near target.
Other Considerations
Contrast sensitivity is a consideration when using distractive or light-splitting lens implants. Contrast sensitivity is already compromised in glaucoma patients, but nondiffractive lenses like the Vivity can generally avoid or eliminate contrast sensitivity–related issues. In addition, a monofocal option like the LAL+ will not affect contrast sensitivity.
It is also important to note that any of these platforms can be combined with MIGS surgeries successfully. The interventional glaucoma revolution has made a very positive impact in surgical results for cataract surgery in our glaucoma patients, because these procedures are mostly surgically neutral and do not change the architecture of the eye significantly. In our clinical practice, we have paired all these IOL platforms with stents and with canaloplasty/goniotomy combinations. In our clinical experience, these minimally invasive techniques do not impact refractive outcomes. This enables us to be more assertive in our offerings, knowing that if premium lens surgery is paired with one of these procedures, we are not negatively impacting their recovery and safety or inducing astigmatism.
In the end, many of these lenses can be effective for our glaucoma patients. It is best as the surgeon to push our own surgical limits and become as comfortable as possible with these platforms while prioritizing candidacy. Patients are relying on us to be the true experts and champions of their vision, and we are lucky in our surgical space to have more options in our toolbox than ever before. GP

References
1. Sarkisian SR Jr, Radcliffe N, Harasymowycz P, et al. Visual outcomes of combined cataract surgery and minimally invasive glaucoma surgery. J Cataract Refract Surg. 2020;46(10):1422-1432. doi:10.1097/j.jcrs.0000000000000317
2. Zhang X, Vadoothker S, Munir WM, Saeedi O. Ocular surface disease and glaucoma medications: a clinical approach. Eye Contact Lens. 2019;45(1):11-18. doi:10.1097/ICL.0000000000000544
3. Vendal Z. Management of glaucoma medication induced dry eye disease with self-retained cryopreserved amniotic membrane. J Dry Eye Ocul Sur Dis. 2022;5(1):e28–e34. doi:10.22374/jded.v5i1.41
4. Vendal Z. Clinical outcomes in patients with mild glaucoma following implantation of violet light–filtering, extended depth-of-focus IOLs. Presented at: ASCRS annual meeting; April 5-8, 2024; Boston.