






Minimally invasive glaucoma surgery (MIGS) has been established in recent years as a safe and effective treatment modality that is ideally situated in the glaucoma treatment paradigm following selective laser trabeculoplasty or topical antiglaucoma medication as a first-line intervention, but prior to invasive filtering surgery.1 Several MIGS devices have been developed in recent years, broadly classified by their site of action into trabecular, subconjunctival, and suprachoroidal procedures.1 Most MIGS devices act on the trabecular meshwork and have a focal approach, such as microtrabecular bypass stents.
However, evidence increasingly indicates that primary open-angle glaucoma (POAG) can be caused by resistance at various levels of the conventional aqueous outflow pathway. Although the trabecular meshwork has been found to contribute roughly 75% of the resistance to aqueous outflow,2 collapse or narrowing of Schlemm’s canal has been found to be responsible for approximately 50% of the decreased outflow facility seen in POAG.3 Further, obstruction of up to 90% of collector channels has also been observed in eyes with POAG.4 Resistance to aqueous outflow thus can arise in the trabecular meshwork (proximal outflow system) as well as Schlemm’s canal and the collector channels (distal outflow system). It is not possible at present to diagnose the exact site of outflow resistance in a patient. Therefore, the efficacy of focal MIGS procedures depends on whether the site of stent placement or tissue removal coincides with the point of obstruction in a glaucomatous eye. This can lead to variable results from patient to patient, with outcomes ranging from large intraocular pressure (IOP) reductions in some to no IOP reduction in others.5 This is reflected in the wide variations seen in the standard deviation of postoperative IOP achieved with focal MIGS procedures, despite a reduction in mean IOP.5-7
Canaloplasty performed via an ab interno surgical technique, commonly referred to as ab interno canaloplasty, is a tissue-sparing and stent-free MIGS.1 It involves 360° catheterization of Schlemm’s canal by a microcatheter, followed by pressurized viscodilation of Schlemm’s canal and the collector channels. Adhesions within Schlemm’s canal are mechanically broken by the circumnavigation of the catheter, and the pressurized viscodilation stretches the trabecular meshwork via the creation of microperforations8 and dilates Schlemm’s canal and the collector channels.9 Importantly, it does so without creating any artificial drainage channels, thus restoring the natural flow of aqueous, which is thought to safeguard against damage to the corneal endothelium.10 Thus, canaloplasty acts comprehensively on the entire conventional outflow pathway, treating multiple possible sites of obstruction in a single procedure. Theoretically, this gives canaloplasty an advantage over focal MIGS procedures in terms of consistency of IOP reduction achieved.
We decided to investigate whether the comprehensive action of canaloplasty translated to consistent eye-by-eye IOP reduction in patients treated with the ab interno technique. The results of our study were recently published in Clinical Ophthalmology.11 This study was the first to focus on eye-by-eye outcomes of any MIGS procedure.
Study Structure and Results
Patients with uncontrolled POAG (preoperative IOP ≥18 mmHg) treated with ab interno canaloplasty with pressurized ophthalmic viscoelastic device (OVD) delivery using the iTrack microcatheter device (Nova Eye Medical) without concomitant cataract surgery were reviewed in a multicenter, multisurgeon, retrospective study. Only patients who had undergone standalone ab interno canaloplasty with pressurized OVD delivery were included, to remove the confounding effect of phacoemulsification on IOP reduction.12 Outcome measures evaluated were reduction in IOP and number of antiglaucoma medications at 12 months. Sixty-four eyes were enrolled with varying grades of glaucoma severity (38% mild, 27% moderate, 27% severe). Six eyes (9%) required additional glaucoma surgery prior to 12 months; these were declared complete failures and subsequently excluded from data analysis.
In the 58 eyes included in the final study cohort, mean IOP (mmHg) dropped from 22.9±7.03 mmHg to 15.0±2.9 mmHg (34% reduction) while mean number of medications dropped from 2.7±0.8 to 1.1±1.1 (58% reduction). Although mean IOP and medication reduction were already expected,13 what was remarkable was the consistency of these outcomes when examined on an eye-to-eye basis.
A consistent reduction in IOP was observed in the cohort, as 57 out of 58 eyes achieved a reduced IOP at 12 months postoperatively (Figure 1). One eye had no change in IOP but achieved a reduction in medications. Of the 57 eyes with reduced IOP, 44 eyes achieved a reduction in both IOP and medications, whereas the remaining 12 eyes achieved a reduction in IOP with the number of medications unchanged from baseline. These were classified as “success” (56 eyes, 88% of entire cohort). One eye out of the 57 reduced-IOP eyes had an increase in the number of medications; this was categorized as “ambiguous,” along with the eye that had no change in IOP but had reduced medications (2 eyes, 3% of entire cohort). No eyes showed an increase in IOP (Figure 2).
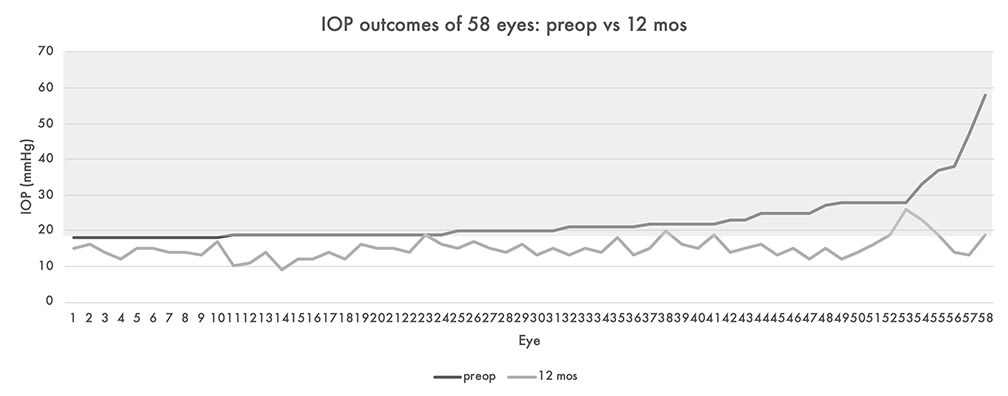
Figure 1. Eye-by-eye intraocular pressure (IOP) outcomes of 58 eyes (preoperative vs 12 months postoperative) receiving canaloplasty. Image courtesy Nova Eye Medical.
IOP reduction ≥20% was observed in 78% of eyes (45/58), and 86% (50/58) eyes achieved IOP ≤18 mmHg (Figure 3). Thus, canaloplasty obtained not only consistent IOP reduction, but also obtained postoperative IOP outcomes consistently below the “safe” limit of 18 mmHg (as recommended by the Advanced Glaucoma Intervention Study).14 Thirty-four percent of eyes (20/58) achieved this safe limit without any medications, compared to none at baseline. Approximately 40% of eyes (23/58) were completely medication-free at 12 months, compared to none at baseline.
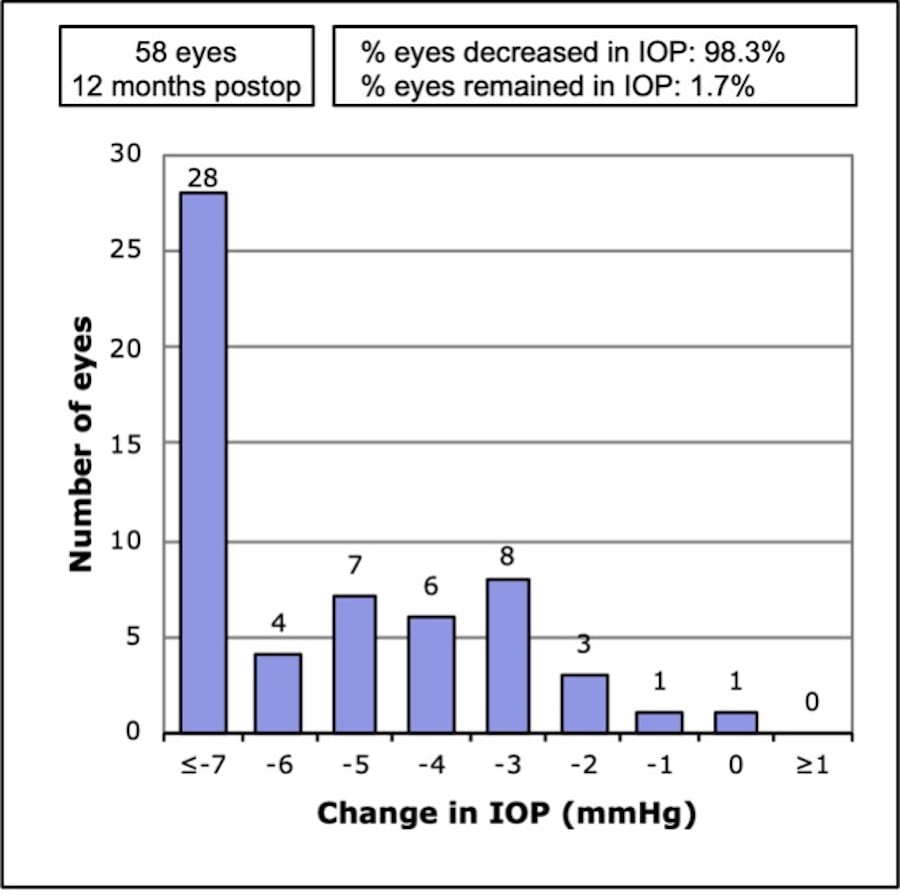
Figure 2. Change in IOP outcomes of 58 eyes (preoperative vs 12 months postoperative) receiving canaloplasty. Image courtesy Nova Eye Medical.
Canaloplasty was effective to varying degrees in most eyes (58/64, 91% of the entire cohort); however, 6 eyes (9%) were excluded from analysis because they underwent additional glaucoma surgery. Although IOP reductions were achieved in some of these eyes, their clinical condition required additional surgical intervention. Secondary surgical intervention rates of 4.5% to 11.3% have been reported after microtrabecular bypass stent surgery.15
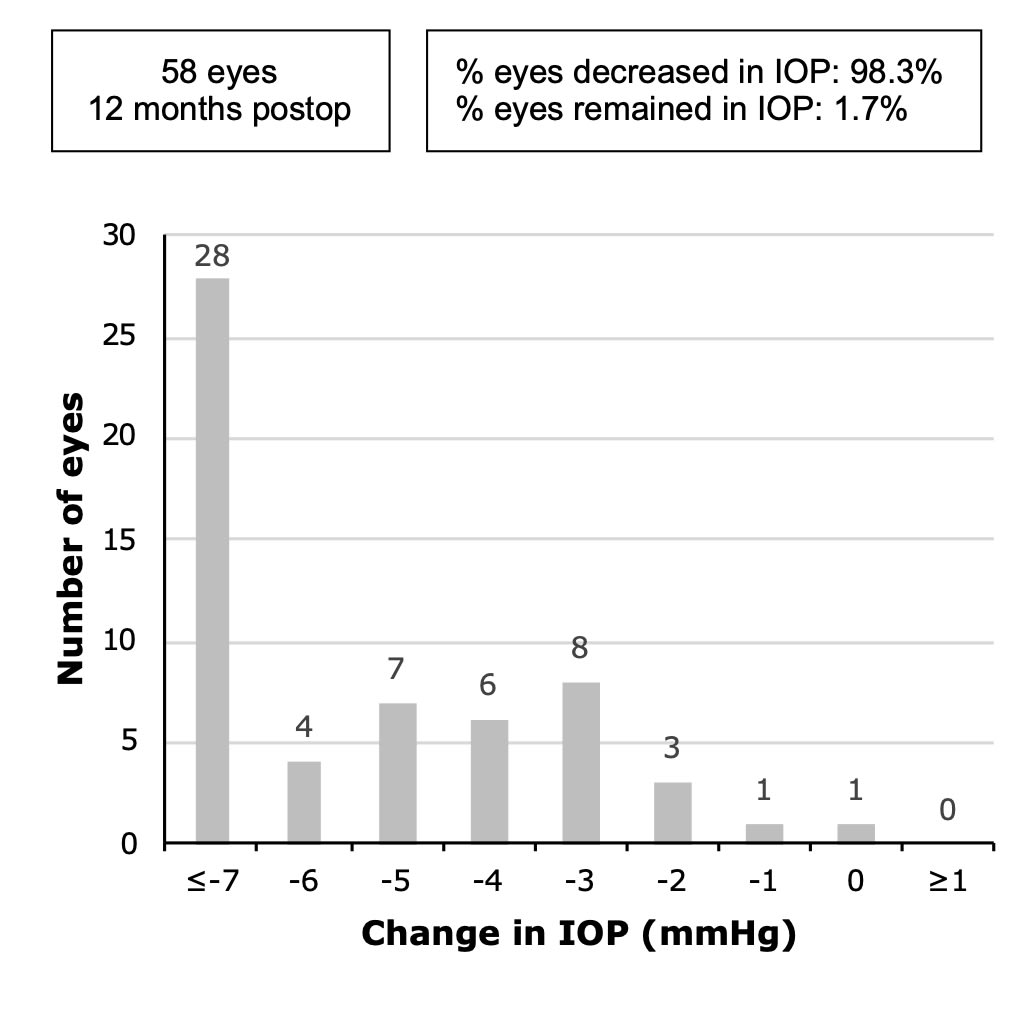
Figure 3. Preoperative and 12-month postoperative distribution of IOP of 58 eyes receiving canaloplasty. Image courtesy Nova Eye Medical.
Conclusion
The study was limited by its retrospective design, lack of randomization, and lack of a control group. However, pooling of data from multiple centers resulted in a diverse cohort in terms of glaucoma stage (mild, moderate, and severe) as well as patient demographics (mean age 71.5±13.4 years; 42% White, 10% Black, 43% Hispanic), which was a major strength of this study.
As the first study to examine consistency outcomes of a MIGS procedure, the results effectively demonstrate that mean IOP reduction should not be the sole metric of treatment efficacy, and that examining the consistency of outcomes on an eye-by-eye basis paints a more accurate picture of the results achieved. Although MIGS is associated with fewer complications than filtering surgeries, it is not without adverse events.1,16 If a procedure is performed on a patient, surgeons must ensure that the results are as predictable, reliable, and repeatable as possible so that most, if not all, patients benefit. This study provides promising evidence that the comprehensive action of canaloplasty achieves consistent and predictable IOP and medication reduction in POAG patients across all stages of glaucoma. GP
References
1. Balas M, Mathew DJ. Minimally invasive glaucoma surgery: a review of the literature. Vision (Basel). 2023;7(3):54. doi:10.3390/vision7030054
2. Grant WM. Further studies on facility of flow through the trabecular meshwork. AMA Arch Ophthalmol. 1958;60(4 Part 1):523-533. doi:10.1001/archopht.1958.00940080541001
3. Allingham R, de Kater AW, Ethier CR. Schlemm’s canal and primary open angle glaucoma: correlation between Schlemm’s canal dimensions and outflow facility. Exp Eye Res. 1996;62(1):101-110. doi:10.1006/exer.1996.0012.
4. Cha EDK, Xu J, Gong L, et al. Variations in active outflow along the trabecular outflow pathway. Exp Eye Res. 2016;146:354-360. doi:10.1016/j.exer.2016.01.008.
5. Arnljots TS, Economou MA. Kahook Dual Blade goniotomy vs iStent inject: long-term results in patients with open-angle glaucoma. Clin Ophthalmol. 2021;15:541-550. doi:10.2147/OPTH.S284687
6. Shalaby WS, Lam SS, Arbabi A, et al. iStent vs iStent inject implantation combined with phacoemulsification in open angle glaucoma. Indian J Ophthalmol. 2021;69(9):2488-2495. doi:10.4103/ijo.IJO_308_21
7. Hengerer FH, Auffarth GU, Conrad-Hengerer I. iStent inject trabecular micro-bypass with or without cataract surgery yields sustained 5-year glaucoma control. Adv Ther. 2022;39(3):1417-1431. doi:10.1007/s12325-021-02039-4
8. Grieshaber MC, Pienaar A, Olivier J, Stegmann R. Clinical evaluation of the aqueous outflow system in primary open-angle glaucoma for canaloplasty. Invest Ophthalmol Vis Sci. 2010;51(3):1498-1504. doi:10.1167/iovs.09-4327
9. Smit BA, Johnstone MA. Effects of viscoelastic injection into Schlemm’s canal in primate and human eyes: potential relevance to viscocanalostomy. Ophthalmology. 2002;109(4):786-792. doi:10.1016/s0161-6420(01)01006-5
10. Lubeck D, Noecker R. Evaluation of endothelial cell density following iTrack ab interno canal-based surgery. Presented at: European Society of Cataract and Refractive Surgeons (ESCRS) 39th annual meeting. October 8-11, 2021; Amsterdam, the Netherlands.
11. Khaimi MA, Koerber N, Ondrejka S, Gallardo MJ. Consistency in standalone canaloplasty outcomes using the iTrack microcatheter. Clin Ophthalmol. 2024;18:173-183. doi:10.2147/OPTH.S441113
12. Shingleton BJ, Pasternack JJ, Hung JW, O’Donoghue MW. Three- and five-year changes in intraocular pressures after clear corneal phacoemulsification in open-angle glaucoma patients, glaucoma suspects, and normal patients. J Glaucoma. 2006;15(6):494-498. doi:10.1097/01.ijg.0000212294.31411.92
13. Khaimi MA. Long-term medication reduction in controlled glaucoma with iTrack ab interno canaloplasty as a standalone procedure and combined with cataract surgery. Ther Adv Ophthalmol. 2021;13:25158414211045751. doi:10.1177/25158414211045751
14. The Advanced Glaucoma Intervention Study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130(4):429-440. doi:10.1016/s0002-9394(00)00538-9
15. Wellik SR, Dale EA. A review of the iStent trabecular micro-bypass stent: safety and efficacy. Clin Ophthalmol. 2015;9:677-684. doi:10.2147/OPTH.S57217
16. Khaimi MA, Dvorak JD, Ding K. An analysis of 3-year outcomes following canaloplasty for the treatment of open-angle glaucoma. J Ophthalmol. 2017;2017:2904272. doi:10.1155/2017/2904272