







For decades, physicians have been aware of the problems that occur when patients fail to adhere to their glaucoma medication regimes,1 as inconsistent drop application results in loss of intraocular pressure (IOP) control, allowing glaucoma to progress. There are many reasons for drop compliance problems, including patient forgetfulness or inability to apply drops properly, cost, supply chain or patient travel challenges, pharmacophobia, and frustration with side effects. Because topical treatment for glaucoma remains a mainstay of the treatment paradigm, alternate ways to ensure medication compliance and reduce untoward side effects have been on the radar for many years.
Pilocarpine, the original drug used to treat glaucoma, requires administration 3 to 4 times a day and is associated with side effects including miosis, brow ache, and blurred vision. To mitigate the dosing schedule and reduce symptoms, slow-release versions of this medication began to be offered in the 1970s, such as pilocarpine hydrochloride ophthalmic gel 4% (Pilopine HS, Alcon) and the pilocarpine ophthalmic ocular insert system (Ocusert Pilo, Alza Corp). These did not take hold. Pilocarpine gel could be irritating to the eye and difficult to administer. The ocular insert could also be difficult to place and often fell out. However, these treatments helped to pave the way for subsequent efforts to provide sustainable, consistent drug delivery, including punctal plugs and a bimatoprost-eluting corneal ring.

Figure 1. Ocusert, a pilocarpine ophthalmic ocular insert system introduced in the 1970s.
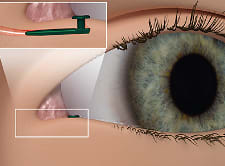
Figure 2. Illustration of the Evolute punctal plug delivery system (Mati Therapeutix).
Intraocular drug delivery offers several advantages over these earlier approaches. Inserts can sustain drug delivery over a long period of time, ensuring that medication reaches the eye consistently. In addition, the tolerability of these systems should not be understated. By avoiding higher concentrations and chronic repetitive doses of topical agents, intraocular drug delivery systems can increase patients’ ocular comfort and reduce adverse external reactions, such as redness, irritation, orbital fat atrophy, or changes in iris color.
Current Drug Delivery Systems
In 2020, the US Food and Drug Administration approved the Durysta bimatoprost intracameral implant (AbbVie), making a viable intraocular drug-delivery platform available. Durysta, although variable in duration of action from 4 months and longer, showed excellent patient acceptance. One of the more significant findings was less ocular irritation, redness, and lid edema noticed by patients in the eyes with the intracameral device.2 Many patients began to realize that all along they had been living with chronic irritation due to the topical agent as compared with the intraocular depot. And this made sense, because the total dose of bimatoprost in a single Durstya implant is 10 µg, which is similar to the dose in each single drop of Lumigan (bimatoprost ophthalmic solution) 0.01% (AbbVie) applied to the ocular surface. However, over a 4-month period, the cumulative total dose of Lumigan to the ocular surface with would be approximately 720 µg as compared to 10 µg in Durysta.

Figure 3. The Durysta bimatoprost intracameral implant was the first intraocular device approved to treat primary open-angle glaucoma.
Recent studies have shown that the duration of action of the Durysta implant could be far longer in some patients, suggesting a remodeling of the outflow pathways with consistent intraocular administration. Depending the severity of the POAG with mild lasting far longer as compared to severe, duration has lasted from as little as 4 months to as long as a year.3 As far as adherence to the treatment schedule, the use of Durysta in the Native American population in Oklahoma has been shown to be well accepted by these patients, who often live extremely far away from pharmacies and medical care.4
Most recently, the FDA has approved the iDose TR system, a tiny canister implanted intracamerally in the angle which releases travoprost over a 2-year duration at a consistent level. This device avoids any trough and peak associated with topical drop therapy and avoids external adverse reactions, such as redness or irritation. No incidents of iris color change or periorbital fat atrophy have been reported. Complications with implantation were rare and no devices needed to be explanted. No device has had to be removed for adverse reaction and no endothelial cell loss occurred over a 5-year period of time even when the device was exchanged in 44 patients and then rechecked at 5 years.
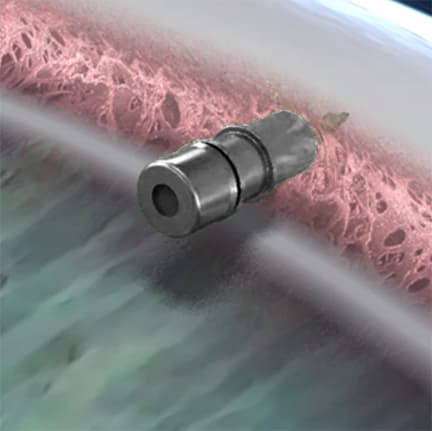
Figure 4. Illustration of the iDose TR intracameral implant, which releases travoprost over a 2-year period.
In a preliminary review, average IOP was lower with the iDose device than with topical travoprost, suggesting no real disadvantage to treatment with the assurance of guaranteed drug adherence.5 Further longer-term data is expected to be released soon.
In our experience in the FDA trial, we found that patients were extremely open to considering iDose TR when they learned it provided continuous therapy, eliminating the need for topical therapy. The 24/365 discussion resonates with patients, particularly those with busy schedules or those who face some of the other barriers to consistent drop administration. Three of the iDose TR clinical sites utilized a clean room modified with filtered air, easily cleaned plastic ceiling tiles, no sink, and linoleum flooring with no corners — all of which allowed for complete cleaning between implantations. Results in these cases were identical to devices placed in surgery centers. These patients showed much less anxiety, knowing they did not need to go to a formal operating room for the implantation procedure.
Systems in Development
Australian biopharmaceutical company PolyActiva is developing PA5108, a biodegradable ocular implant that releases latanoprost over a 6-month period. Interim results from a phase 2a study conducted in Australia and New Zealand demonstrated a sustained >20% reduction of IOP after 6 months with a favorable safety profile. Eight out of 17 subjects were successfully dosed with a second implant at 21 weeks, providing ongoing, uninterrupted therapy.6 The company says it plans to initiate a phase 2b clinical trial in the United States, Australia, and New Zealand during 2024.
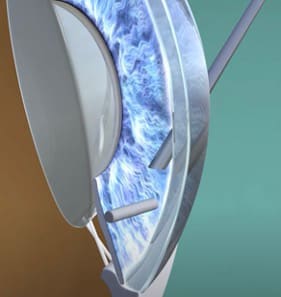
Figure 5. An injector will deliver PA5108, a biodegradable ocular implant being developed in Australia by PolyActiva.
Another drug-delivery device currently being developed is Paxtrava (formerly OTX-TIC, Ocular Therapeutix), a travoprost intracameral implant which, like Durysta, is injected into the anterior chamber.7 The company recently reported positive topline 6-month data, which included a reduction in mean IOP of 24% to 30% from baseline. Also, 81.3% of implant-treated eyes did not require additional IOP-lowering therapy, suggesting sustained and consistent treatment effects.8
The SpyGlass Pharma drug delivery platform consists of a single-piece, hydrophobic acrylic intraocular lens (IOL), with drug-eluting reservoir pads attached to the haptics. After implantation during cataract surgery, the system is designed to elute bimatoprost for up to 3 years. Unlike the Durstya or iDose TR implants or dissolvable devices, the SpyGlass drug reservoirs do not change shape or size over time, so there is no effect on IOL position, and the reservoir pads are outside the visual axis. The SpyGlass IOL is currently being evaluated in an FDA phase 2 trial.9
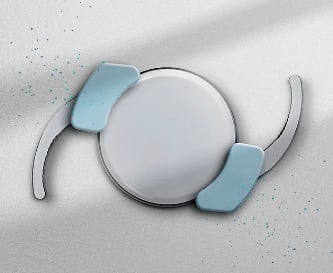
Figure 6. The SpyGlass drug delivery intraocular lens is currently being tested in a clinical trial.
Conclusion
The pipeline for intraocular drug delivery devices to treat glaucoma is both full and promising. Patients in poor, rural, or underserved areas, as well as populations in the developing world, will benefit from the consistent treatment these devices provide. One can look forward with anticipation to more choices as companies race to a drop-free future.
Other medications such as rho kinase inhibitors, may be suitable for intraocular inserts to avoid the medication-related side effects of topical dosing. Longer-acting devices would be possible simply by increasing the size of the device to permit greater drug volume. If 2 molecules could coexist in a single device, combination devices could provide better IOP control and further drop reduction. Or, if combination devices prove unfeasible, separate devices each with different medications might work together in a similar way. There may also be opportunities for other minimally invasive procedures to be done at the same time as drug device insertion, permitting multiple mechanisms or pathways for aqueous outflow.
It should be emphasized that none of these devices would have been possible without advances in the MIGS space. Nor would they have become reality without the strenuous efforts of the manufacturers, their engineers, and pioneer clinicians who committed so much time, effort, and financial support to insist on better options even in the face of resistance to change. GP

References
1. Kass MA, Meltzer DW, Gordon M. A miniature compliance monitor for eyedrop medication. Arch Ophthalmol. 1984;102(10):1550-1554. doi:10.1001/archopht.1984.01040031266033
2. Ali AA, Avilés Elescano D, Grover DS. Bimatoprost SR for glaucoma therapy implanted at the slit-lamp in a real-world Setting. Clin Ophthalmol. 2024;18:1371-1377. doi:10.2147/OPTH.S450220
3. Teymoorian S, Craven ER, Nguyen L, Werts E. Real-world study of the effectiveness and safety of intracameral bimatoprost implant in a clinical setting in the United States. Clin Ophthalmol. 2024;18:187-199. doi:10.2147/OPTH.S445005
4. Sarkisian SR Jr, Mitchell EC. Real-world analysis of the efficacy of bimatoprost sustained-release glaucoma implant where American Indians comprise the largest minority population. Clin Ophthalmol. 2024;18:917-927. doi:10.2147/OPTH.S452159
5. Glaukos announces positive topline outcomes for both phase 3 pivotal trials of iDose TR, achieving primary efficacy endpoints and demonstrating favorable tolerability and safety profiles. News release. September 7, 2022. Accessed July 31, 2024. https://investors.glaukos.com/investors/news/news-details/2022/Glaukos-Announces-Positive-Topline-Outcomes-for-Both-Phase-3-Pivotal-Trials-of-iDose-TR-Achieving-Primary-Efficacy-Endpoints-and-Demonstrating-Favorable-Tolerability-and-Safety-Profiles/default.aspx
6. PolyActiva reports promising clinical trial results for its 6-month sustained drug delivery, biodegradable ocular implant in glaucoma patients. News release. November 2, 2023. Accessed July 30, 2024. https://polyactiva.com/wp-content/uploads/2023/11/PolyActiva-Phase-2-Results-US.pdf
7. A study to evaluate the efficacy and safety of OTX-TIC (travoprost) intracameral implant for patients with open-angle glaucoma (OAG) or ocular hypertension (OHT). ClinicalTrials.gov Identifier: NCT05335122. Updated December 12, 2023. Accessed July 30, 2024. https://clinicaltrials.gov/study/NCT05335122
8. Ocular Therapeutix announces positive phase 2 Paxtrava glaucoma data at the American Society of Cataract and Refractive Surgery 2024 annual meeting. News release. April 6, 2024. Accessed July 30, 2024. https://www.globenewswire.com/news-release/2024/04/06/2858799/0/en/Ocular-Therapeutix-Announces-Positive-Phase-2-PAXTRAVA-Glaucoma-Data-at-the-American-Society-of-Cataract-and-Refractive-Surgery-2024-Annual-Meeting.html
9. Evaluation of the bimatoprost implant system used in combination with the SpyGlass intraocular lens compared to timolol ophthalmic solution (Tigris). ClinicalTrials.gov Identifier: NCT06120842. Updated November 13, 2023. Accessed July 30, 2024. https://clinicaltrials.gov/study/NCT06120842