







Climate change represents a major health threat to humanity, so ophthalmologists must be mindful of their carbon footprint in the operating room, warned Aakriti Garg Shukla, MD, MSc, during the recent meeting of the American Glaucoma Society (AGS) in Washington, DC.

“Climate change resulting from deforestation and industrialization is something that should concern all of us as residents of planet earth, but this topic becomes increasingly relevant when we realize the impact we’re having on a daily basis as physicians and surgeons,” observed Dr. Shukla, the Leonard A. Lauder Associate Professor of Ophthalmology at Columbia University in New York City (Figure 1). “Every surgery generates 1 or more large trash bags, and if you’re a typical surgeon doing 10 to 15 cases in a day, your operating room (OR) day has generated the waste equivalent of 2 to 4 months of a household’s trash. Much of this must be disposed of as regulated health care waste, further increasing the environmental burden.”
Fortunately, Dr. Shukla explained, there are numerous ways to make cataract and glaucoma surgery more sustainable, protecting the environment while maintaining high standards for patient care.
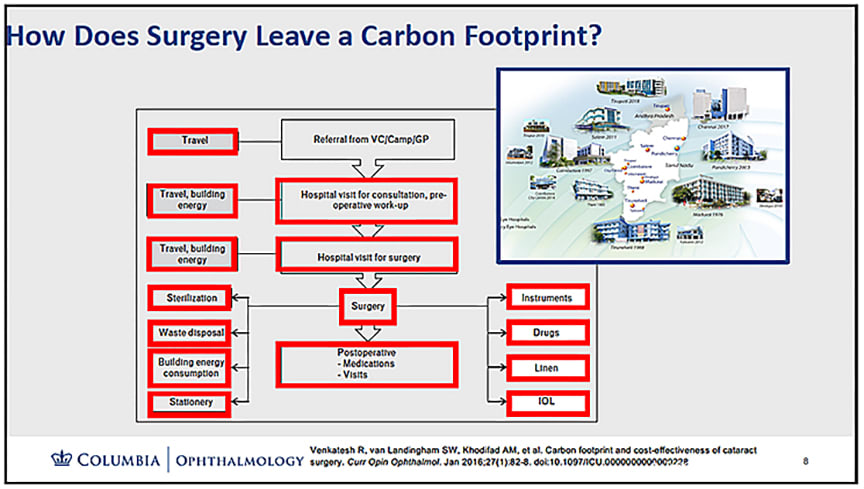
Figure 1. Every aspect of glaucoma treatment—from patient and staff travel for preoperative, operative, and postoperative visits to the energy used in medical facilities, the production and transportation of surgical instruments, drugs, linens, drapes, and implants, and ultimately the disposal of medical waste—contributes to its overall carbon footprint. Image courtesy Aakriti Garg Shukla, MD.
Reducing Operating Room Waste
One of the most effective strategies for reducing waste in glaucoma surgery is to reevaluate the necessity of certain instruments and supplies. Dr. Shukla recommended a “2-week challenge,” during which an observer, such as a medical student or nurse, keeps track of instruments and items in the surgical pack that were not used in each procedure. By the end of the 2 weeks, surgeons will have data they can use to eliminate unnecessary or rarely used items from their tray.
Surgical techniques can also be modified to be more sustainable. For example, Dr. Shukla highlighted a leaner alternative to traditional goniotomy: “Bent needle–assisted goniotomy uses a single-use, minimally packaged needle instead of a commercial goniotomy blade, which can cost around $350.” Similarly, in gonioscopy-assisted transluminal trabeculotomy (GATT), surgeons can use a simple Prolene suture instead of a disposable plastic device, she said, cutting down on both waste and expense.
Surgical draping is another potential area for waste reduction. Rather than draping the entire patient, she suggests using face and neck drapes to cover the area around the surgical site. This reduces material use without compromising sterility or patient safety. “Surveys of ophthalmologists have found that about 45% have eliminated the full-body drape during eye surgery,” Dr. Shukla noted.
Sustainable Medication Practices
Pharmaceutical waste is another significant contributor to environmental harm, with ophthalmology also facing numerous drug shortages. A major issue is the widespread practice of discarding single-use eye drop bottles that still contain a large volume of medicine. Dr. Shukla cited a multisociety position paper written by Alan Robin, MD, and David Palmer, MD, which recommended that topical drugs in multidose containers be used across multiple patients and kept until their expiration date, rather than being arbitrarily discarded after 28 days.1 The paper also recommended that after surgery, patients should be able to bring their partially used medication home for postoperative use.
Microdosing of ophthalmic medications is another promising solution. “Microdrops, which deliver 1/40th the volume of a standard drop, have been found to be noninferior in intraocular pressure lowering and pupillary dilation,” said Dr. Shukla. These smaller drops not only reduce drug waste but may also decrease systemic side effects (Figure 2).
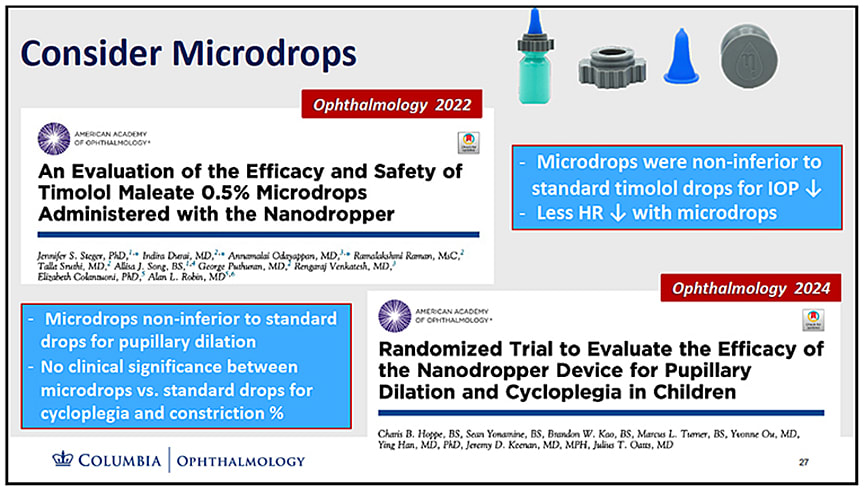
Figure 2. Clinical trials have validated the efficacy and safety of glaucoma microdrops, which may improve patient adherence by reducing adverse effects associated with larger doses of medications. Image courtesy Aakriti Garg Shukla, MD.
Rethinking Clinic Visits and Equipment Use
In clinical practice, reducing unnecessary patient visits can also lessen the environmental footprint. Dr. Shukla suggested performing procedures like laser peripheral iridotomy (LPI) or selective laser trabeculoplasty (SLT) bilaterally when indicated, allowing patients to avoid multiple trips. Remote monitoring technologies, such as home tonometry and virtual visual fields, can also reduce travel-related emissions for glaucoma suspects or for patients whose disease is stable and well managed, she added.
Single-use diagnostic tools are another target for reform. While infection prevention is paramount, many devices currently used once and discarded—such as tonometer tips and gonioscopy lenses—could be replaced with reusable options that can easily and safely be disinfected between patients. Dr. Shukla emphasized that guidelines from the Centers for Disease Control and Prevention (CDC) and the American Academy of Ophthalmology (AAO) support such practices.
Industry and Policy Changes
Beyond individual practices, broader systemic changes are needed to make ophthalmology more sustainable. Dr. Shukla encouraged ophthalmologists to advocate for manufacturers to transition to reusable devices, such as goniotomy blades, SLT lenses, and surgical probes.
She also called for the adoption of electronic instructions for use (IFUs) instead of the bulky paper inserts that accompany medical devices. “Most of us are not looking at a piece of paper once we’re scrubbed in,” she noted, highlighting the inefficiency of the current system. Dr. Shukla was a coauthor of a recent white paper led by Dr. Emily Schehlein that recommended manufacturers begin replacing printed IFUs with QR codes that link to online electronic instructions for use (e-IFU), which can be easily accessed by surgeons in the clinic, while also reducing emissions and printing costs.2
For more information on sustainability in ophthalmology, visit EyeSustain.org, a collaboration of the American Academy of Ophthalmology (AAO), the American Society of Cataract and Refractive Surgery (ASCRS), and the European Society of Cataract and Refractive Surgery (ESCRS). The site provides resources to help make ophthalmology more sustainable, both economically and environmentally.
Online resources, such as EyeSustain.org, provide additional guidance for environmentally conscious ophthalmologists. The website, supported by AGS, the American Academy of Ophthalmology (AAO), the American Society of Cataract and Refractive Surgeons (ASCRS), and many other organizations, offers practical tools such as a carbon footprint calculator for operating rooms and strategies for implementing greener practices.
Conclusion
While the challenges of reducing waste in glaucoma surgery are significant, they are not insurmountable (Figure 3). Surgeons can take steps to reduce waste in the short term, and advocate for long-term goals, such as regulatory changes and industry-wide adoption of sustainable devices and practices. “Ophthalmologists are deeply committed to reducing their environmental impact,” concluded Dr. Shukla. “We have the knowledge and the tools to make meaningful changes—now it’s up to us to act.” GP
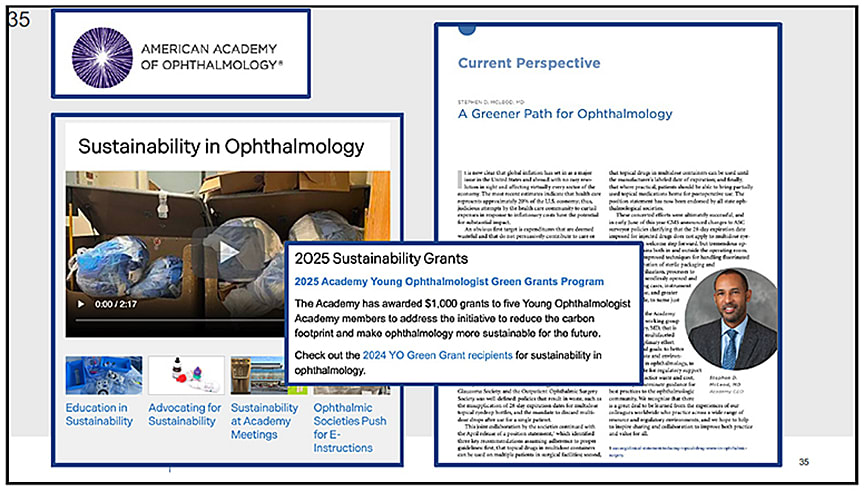
Figure 3. With the goal of making ophthalmology more sustainable, each year the American Academy of Ophthalmology provides $1,000 “Green Grants” to young ophthalmologists for research into sustainable solutions. Image courtesy Aakriti Garg Shukla, MD.
References
1. Palmer DJ, Robin AL, McCabe CM, Chang DF; Ophthalmic Instrument Cleaning and Sterilization Task Force. Reducing topical drug waste in ophthalmic surgery: multisociety position paper. J Cataract Refract Surg. 2022;48(9):1073-1077. doi:10.1097/j.jcrs.0000000000000975
2. Schehlein EM, Hovanesian J, Shukla AG, Talley Rostov A, Findl O, Chang DF. Reducing ophthalmic surgical waste through electronic instructions for use: a multisociety position paper. J Cataract Refract Surg. 2024;50(3):197-200. doi:10.1097/j.jcrs.0000000000001381