







For decades, traditional glaucoma surgery focused on creating a new drainage system for the eye, abandoning the natural outflow system. In the past 2 decades, with improvements in technology and devices, enhancing flow through the natural aqueous drainage pathways became possible with minimally invasive glaucoma surgery (MIGS) procedures. From trabeculectomy to tube shunts and, more recently, canal-based MIGS, the field has evolved through continual innovation, emphasizing safety to approach the disease, especially noteworthy with early disease. Yet even as techniques improve, the goal remains the same: to safely lower intraocular pressure (IOP) by restoring or enhancing physiologic outflow.
At Glaucoma Associates of Texas (GAT), we have long embraced a culture of innovation—developing, refining, and challenging surgical approaches to help patients manage this chronic disease. Building on our experience with canal surgery and the knowledge gained from gonioscopy-assisted transluminal trabeculotomy (GATT), we have introduced a new procedure: interventional valve-enhancing trabeculotomy, or iVEnT. This technique is designed to be less invasive and preserve the intracanalicular structures of Schlemm’s canal with the hope of improving pulsatile outflow through physiologic collector channels. Our surgical concept was heavily influenced by the work of Murray Johnstone, MD, who described the pulsatile motion of intracanalicular structures involved in aqueous outflow.

Figure 1. Microspatula invented for the iVEnT procedure, with the edge angled to make cuts to the left. Image courtesy Glaucoma Associates of Texas.
In this article, we introduce the iVEnT procedure, discuss the rationale for its development, describe the surgical technique, and share early clinical experiences. Our aim is to equip glaucoma surgeons with the knowledge and context needed to evaluate whether iVEnT may fit into their surgical armamentarium.
Origins and Evolution Toward iVEnT
The journey to iVEnT began with GATT. When we first introduced GATT, it opened new possibilities for circumferential trabeculotomy performed from an ab interno approach.1 The procedure demonstrated that effective IOP reduction could be achieved by fully incising the trabecular meshwork (TM), restoring communication between the anterior chamber and Schlemm’s canal.
Over time, as we carefully studied GATT results and performed thousands of cases, patterns emerged. Some patients achieved excellent IOP reduction, while others experienced more modest outcomes despite technically successful procedures. This variability suggested that factors beyond the TM itself—particularly the distal outflow system—play a critical role in surgical success.
Traditional teaching often depicts aqueous humor outflow as a simple pressure-driven process. Yet physiologic studies and intraoperative observations reveal a more nuanced picture. As Johnstone and others have noted, outflow through Schlemm’s canal is pulsatile, linked to the cardiac cycle and venous pressure changes (Video 1).2
Theoretically, the valves within Schlemm’s canal act as dynamic structures, regulating and directing aqueous fluid into collector channels and preventing reflux. When these valves lose function, possibly related to loss of outflow tissue elasticity, the outflow system becomes inefficient. In glaucoma, particularly open-angle glaucoma, evidence suggests that valve dysfunction contributes significantly to elevated IOP. Enhancing or restoring valve function could therefore represent an important therapeutic strategy. With iVEnT, the surgical goal is to cleave the TM in a manner that specifically is designed to avoid trauma to the valves and potentially enhance pulsatile outflow, rather than relying solely on bulk flow through a wide trabeculotomy opening.
How iVEnT Is Performed
The iVEnT procedure shares some similarities to GATT, but there are important differences. To perform iVEnT, we invented a pair of small microspatulas with cutting edges: one is angled to make cuts to the left, the other is angled to make cuts to the right (Figure 1). We spent a lot of time and effort fine-tuning these instruments so they would cause minimal trauma to the angle while still allowing us to make precise incisions.
After creating a standard ab interno approach through a clear corneal incision, the surgeon advances the left-angled microspatula across the anterior chamber to the nasal angle, using it to create a precise incision through the nonfiltering portion of the TM, just below Schwalbe’s line. This incision site may also reduce unwanted wound healing. Depending on the patients’ level of disease, the incision can be 90° or 120° (3 to 4 clock hours) or more. Then the left-angled tool is withdrawn, and the right-angled microspatula is inserted and used to cleave the nonfiltering TM in the other direction (Video 2).
These incisions should be as superficial as possible, and only one pass is used in each direction. The cleavage plane initiated below Schwalbe’s line extends slightly into the nonfiltering TM, and at the same time the incision plane extends into the very superficial anterior part of Schlemm’s canal, away from the location of the valves, which are typically located in the posterior part of the canal.
When performing the procedure, Schwabe’s line is a key landmark. The incision should be made just posterior to this line, with the instrument directed toward the pupil to ensure precision incision of the most anterior TM without entering the canal and potentially harming intracanalicular structures. By maintaining an anterior trajectory and consistently pulling toward the pupil, surgeons can control the depth and placement of the incision. Because the procedure employs a microscopic instrument and doesn’t go deeply into TM or the canal, bleeding is minimal and visualization remains clear. This makes the technique relatively straightforward to perform (Video 3).
This approach minimizes disruption of intracanalicular structures and incisional damage to the TM, which may help reduce scarring while maintaining structural support. Gonioscopic visualization and steady hand control are critical, but surgeons who are already familiar with angle surgery and GATT should find the transition manageable once they adapt to the targeted incision strategy.
Early Outcomes
Thus far, iVEnT has shown promising results. Data presented at the 2025 American Glaucoma Society meeting showed that 218 eyes with moderate to advanced glaucoma that underwent iVEnT showed a statistically significant and sustained reduction in IOP, falling from a mean preoperative IOP of 16.2 mmHg to 13.5 mmHg at 6 months after surgery (a 13.3% reduction) and 13.4 mmHg at 24 months (a 12.4% reduction).3
This reduction was accompanied by a sharp drop in glaucoma medications, from a preoperative average of 2.18 medications to a postoperative average of 0.61 medications at 6 months (64.5% reduction) and 0.79 medications at 24 months (60.1% reduction). At last visit, patients averaged 0.68 medications, representing a 66.8% reduction compared with baseline. Both the drop in IOP and the reduction in medications were statistically significant at all time points (P<.001). Importantly, more than 50% of these patients, regardless of the starting pressure, ended up on no medications and their pressures were in the low teens (Figure 2).
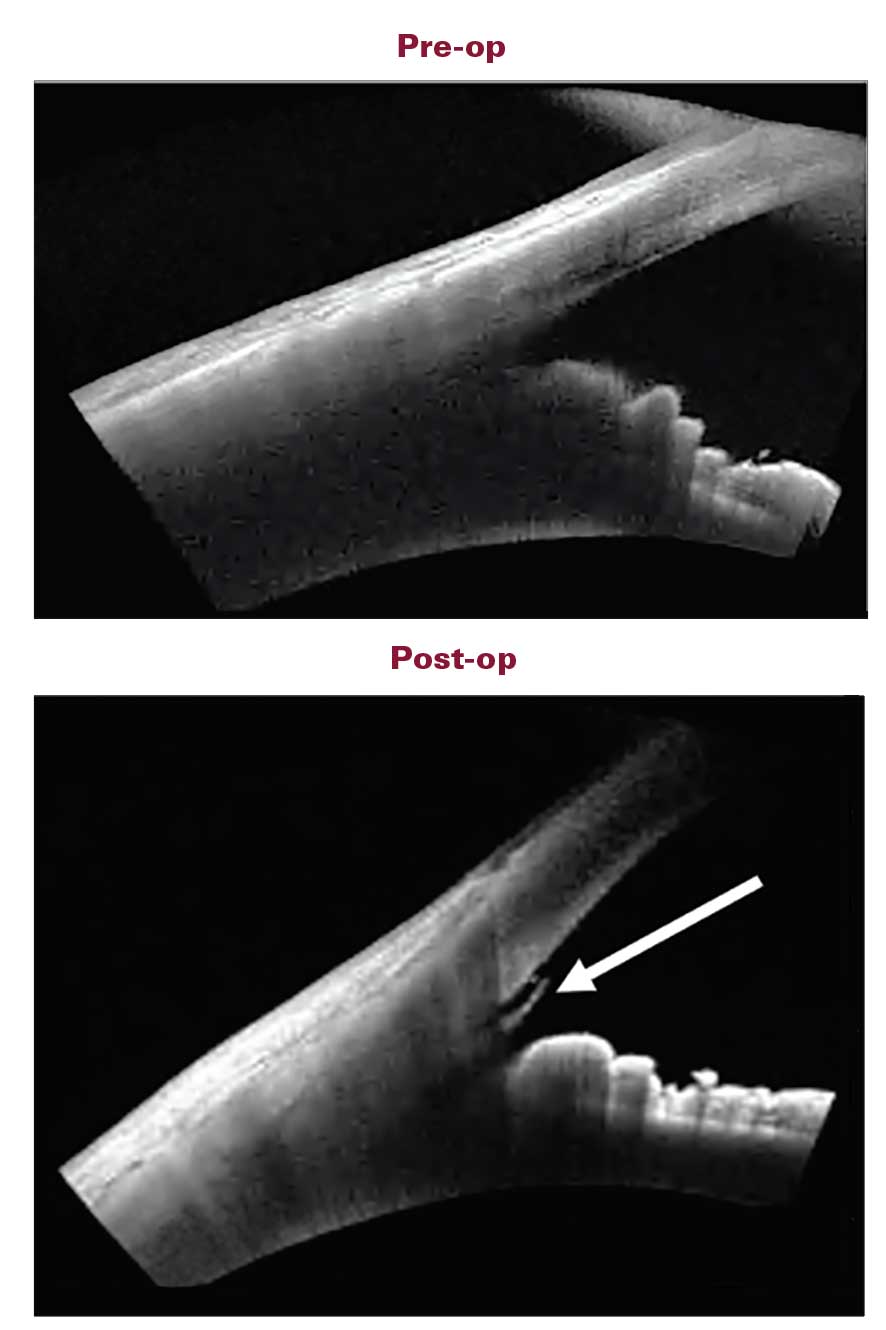
Figure 2. Following the iVEnT procedure, outflow tissue is realigned, reopening collapsed trabecular meshwork lamellae and dilating Schlemm’s canal. As indicated by the arrow, increased outflow causes the trabecular meshwork and Schlemm’s canal to bow inward, which expands the circular deep scleral plexus, enhances flow to the distal collector channels, and promotes pulsatile outflow. Image courtesy Glaucoma Associates of Texas.
Overall, complications were relatively uncommon beyond the early postoperative period. The procedure avoids bleb-related complications such as leaks and late infections, and avoids placing hardware in the anterior chamber, potentially reducing risks of corneal decompensation.
Although these observations are encouraging, it is important to emphasize that iVEnT remains in its early stages. Rigorous clinical studies with long-term follow-up are needed to validate efficacy, safety, and durability compared to established procedures, and determine the role iVEnT will play relative to other MIGS options or combined cataract surgery.
Conclusion
Glaucoma surgery continues to advance through a combination of observation, persistence, and the need for something better. iVEnT reflects these values: a procedure born from clinical insights from surgeons and researchers, designed to target the overlooked role of Schlemm’s canal valves, and performed with the goal of restoring pulsatile outflow. Our early experience suggests that iVEnT may offer a new way forward for patients who need effective pressure control without the risks of filtering surgery. As we continue to refine this technique, our hope is that it will empower glaucoma specialists with another tool to help patients preserve vision and quality of life. GP


Editor's note: Drs. Fellman and Grover are the inventors of the microspatula used in the iVEnT procedure and hold a patent related to its design. It is not yet commercially available.
References
1. Grover DS, Godfrey DG, Smith O, Feuer WJ, Montes de Oca I, Fellman RL. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: technique report and preliminary results. Ophthalmology. 2014;121(4):855-861. doi:10.1016/j.ophtha.2013.11.0012
2. Johnstone MA. The aqueous outflow system as a mechanical pump: evidence from examination of tissue and aqueous movement in human and non-human primates. J Glaucoma. 2004;13(5):421-438. doi:10.1097/01.ijg.0000131757.63542.24
3. Grover DS. Glaucoma surgery day lecture: Are we doing our best: a vision for continued growth. Presented at: American Glaucoma Society meeting; February 27, 2025; Washington, DC.