Gonioscopy remains a critical examination technique for ophthalmologists to visualize the anterior chamber angle. In clinical practice, it is the standard of care for evaluating patients with glaucoma or suspected glaucoma, because it helps identify open or closed angles, distinguish between appositional and synechial angle closure, and diagnose secondary glaucomas such as pigmentary, pseudoexfoliative, or traumatic glaucoma. (Figure 1).

Figure 1. Four-mirror gonioscopy photograph showing iridodialysis following blunt ocular trauma. Iridodialysis can generally be distinguished from cyclodialysis on gonioscopy by the color of the cleft space: in iridodialysis, the space is usually pigmented due to residual iris tissue, whereas in cyclodialysis it appears white, reflecting exposed sclera after the uveal tissue has detached.
Evaluating the status of the angle helps inform clinical treatment decision-making, as well as procedural or surgical planning. The American Academy of Ophthalmology Preferred Practice Patterns specifically recommends using gonioscopy in the initial exam and as needed in follow-up evaluations for primary open-angle glaucoma, primary angle-closure glaucoma, and certain retinal disorders that could lead to neovascularization of the angle, as well as for perioperative planning.1 Despite this, a 2006 study reported that only 49% of Medicare beneficiaries undergoing glaucoma surgeries had a documented gonioscopic exam in the 4 to 5 years proceeding their surgery.2 Ophthalmologists must ensure that they continue to follow current recommendations and include gonioscopy into their clinical exam. Furthermore, in the operating room, intraoperative gonioscopy is a skill required to visualize and perform angle-based surgical procedures, especially as minimally invasive glaucoma surgeries (MIGS) continue to increase in use.
Viewing the Angle and Types of Lenses
The structures of the anterior chamber angle are not visible to the unaided eye due to the total internal reflection that occurs at the surface of the eye.3 Many different types of gonioscopy lenses exist to overcome this optical difficulty, categorized as direct lenses and indirect lenses. In indirect gonioscopy, light rays are reflected by a mirror in the contact lens to overcome the total internal reflection.3 In direct gonioscopy, the steeply convex anterior curve of the lens allows for refraction of light from the angle to exit the eye.3
Gonioscopy in the Clinic

Figure 2. Large diameter 3 mirror gonioscopy lens used for angle and peripheral retina viewing.
In the clinic, indirect gonioscopy lenses are typically used; these allow for visualization of the angle structures with the patient in an upright position at the slit lamp. The view is an inverted image of the opposite angle due to the reflection of light. Indirect gonioscopy lenses include the Posner, Zeiss, Sussman, and Goldmann lenses. The Posner and Zeiss lenses contain 4 identical mirrors, which allow for 360° viewing of the angle with minimal rotation of the lens. The lens is held by its rod-shaped handle, and the 9-mm central area contacts the cornea without need for a coupling agent.3 Its small contact area facilitates indentation gonioscopy, where pressure on the lens can deepen the angle and allow for dynamic viewing. The Sussman is similarly a 4-mirror lens but is held directly by the examiner without a handle.3 The Goldmann 3-mirrored lens has 2 mirrors to examine the peripheral retina and 1 lens tilted to examine the angle (Figure 2). This lens is used with a viscous coupling agent, and its larger 12-mm central area may artificially close the angle with applied pressure, making indentation gonioscopy challenging with this lens.

Figure 3. Proper placement of a 1-mirror laser trabeculoplasty gonioscopy lens. The lens should be rotated through 360° during laser application.
Trainees and newer practitioners may struggle with the gonioscopy technique. In the clinic, there are a few practical steps that may help with performing this procedure:
- Ensure the patient is comfortable and positioned appropriately in the slit lamp. Apply topical anesthetic to numb the patient’s eye.
- Keep the room dimly lit and use a shorter slit lamp beam, which will prevent the pupil from constricting, thus making any iridotrabecular contact more apparent.
- Use a coupling agent such as artificial tear gel.
First, instruct the patient to look upwards, and place the inferior aspect of the gonioscopy lens on the inferior sclera. Ask the patient to look straight ahead, then tip the lens forward to make full but gentle contact with the surface of the patient’s eye. Make sure the patient keeps both eyes open and is now looking forward; try to keep the lens as perpendicular as possible (Figure 3).
Remember that the viewing mirror is 180° away from the visualized angle. Proceed in a systematic fashion—many practitioners will start with the inferior angle, because it is often the widest, and then proceed clockwise. Proper visualization takes practice, and sometimes small adjustments are necessary, such as asking the patient to look toward the mirror of evaluation or tilting the lens in the direction of the angle to be viewed.
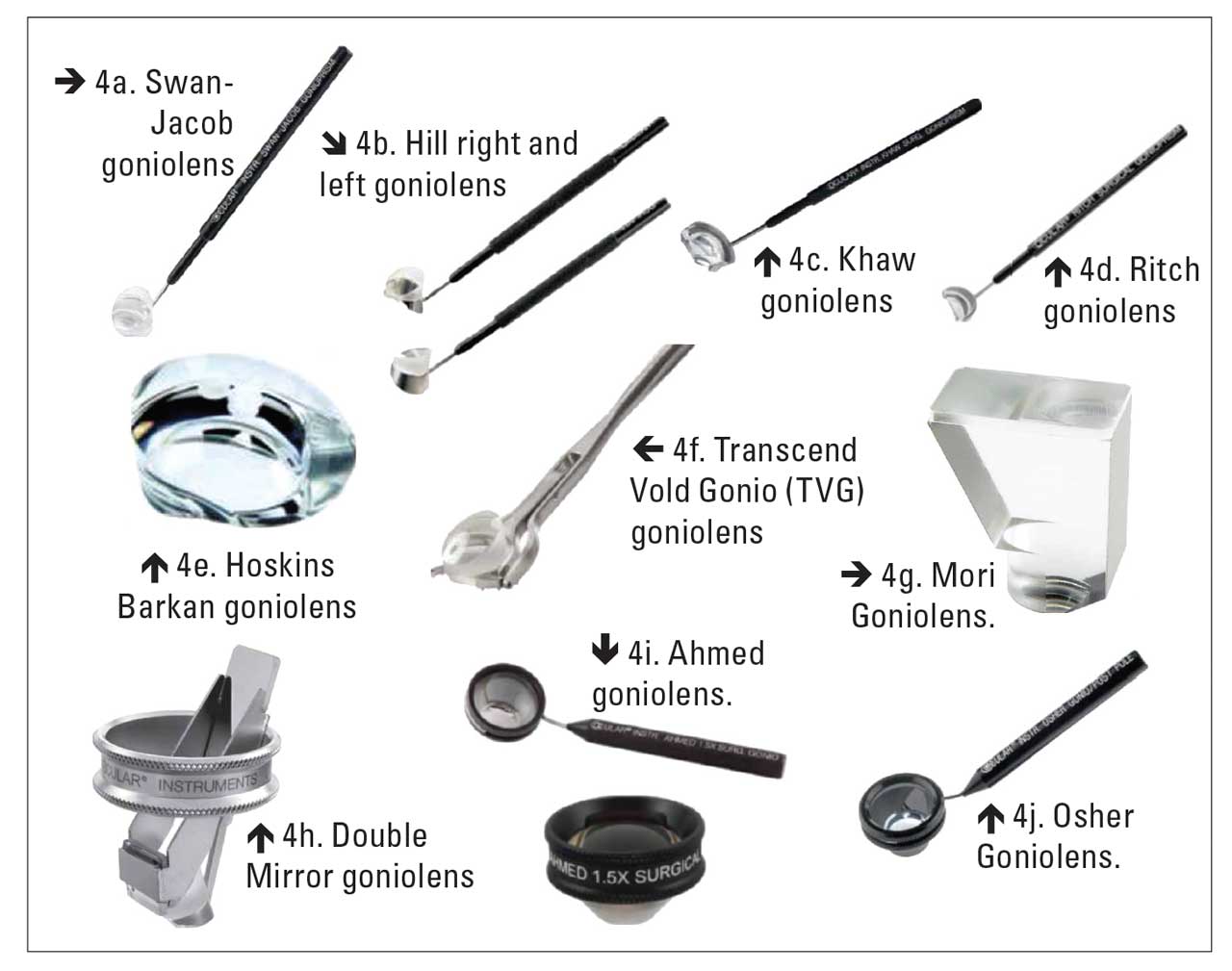
Figure 4. A variety of gonioscopy lenses.
Gonioscopy in the Operating Room
Direct gonioscopy lenses, such as the Koeppe lens and Swan-Jacob lens (Figure 4a), are commonly used in the operating room when the patient is supine. They allow for direct visualization of the angle, producing an erect, noninverted image of the target angle. The Koeppe lens is very commonly used for evaluation of children, often with the use of a portable slit lamp in the other hand.3 The Swan-Jacob gonioscopy lens typically has an attached rod to allow for manipulation during intraoperative procedures and require use of a coupling agent.3
Many surgical gonioscopy lenses are variations of the Swan-Jacob design, such as Hill, Khaw, and Ritch lenses (Figures 4b, 4c, 4d), differing in fixation support, field of view, corneal contact, and handle length.4 Direct-viewing lenses, including Hoskins Barkan and Transcend Vold Gonio (TVG), provide fields of view from 90° to 360° and magnifications of 0.73x to 1.50x (Figures 4e, 4f).4 However, most require tilting the patient’s head or the surgical microscope by 30° to 40°, which can be ergonomically challenging and time-consuming.4 Designs like Hill and TVG incorporate stabilization features such as flanges or cleat rings, although these can cause patient discomfort and subconjunctival bleeding.4
Dual-viewing lenses, such as the Mori (Figure 4g) and Double Mirror (Figure 4h), use internal mirrors to enable coaxial visualization, eliminating the need for head or microscope tilting and allowing surgeons to maintain a neutral posture.4 The Mori lens uniquely allows simultaneous visualization of the anterior chamber angle and the anterior chamber, but can cause significant minification, making detailed surgical maneuvers more difficult.4 Dual-viewing lenses suffer from reduced light transmission and lack adequate globe stabilization mechanisms, potentially increasing surgical risk from involuntary eye movements.4
Indirect-viewing lenses, including Ahmed and Osher, offer high magnification and ergonomic advantages (Figures 4i, 4j).4 The Ahmed lens provides 1.5x magnification—the highest among surgical goniolenses—and allows 360° rotation without moving the patient or microscope.4 Both Ahmed and Osher lenses enable corneal contact rotation for complete angle visualization.4 However, their inverted images require spatial reorientation and surgical dexterity, increasing the learning curve and risk of inadvertent trauma.4
Optimizing visualization into intraoperative gonioscopy is critical to ensure that all surgical instruments approach the target tissue plane en face and parallel to the iris plane. Proper setup begins with proper positioning. To visualize the nasal angle, the patient’s head is rotated nasally, and the microscope is rotated towards the surgeon. The exact amount of rotation may vary from surgeon to surgeon but typically ranges from 30° to 45°. The microscope arm can be marked with tape at the desired angle so that the microscope is rotated the same amount each time.
Note that this rotational movement will displace the surgical field and increase the working distance between the microscope oculars and the patient’s eye, sometimes resulting in excessive surgeon neck and back flexion. As ophthalmologists have reported a higher prevalence of musculoskeletal pain related to the workplace, maintaining proper ergonomic positioning during angle surgery is crucial.5 One tip during positioning is to lower the chair and lift the oculars to maintain a vertical posture and primary gaze. Manually lower the microscope when refocusing to maintain the full range of focus.
If the surgical gonioscopy lens has a handle, it is held in the nondominant hand, with the surgeon using the side of that hand on the patient’s face as a stabilizing and pivot point for gentle lens docking and manipulation. Surgical gonioscopy lenses without a handle (“hands-free” lenses) typically have a wider stabilizing base and can be placed on the eye and occasionally manipulated or lightly stabilized with the surgeon’s nondominant finger as needed. Choice of intraoperative gonioscopy lens ultimately depends on the surgeon’s experiences and preference.
Visualization of anatomical structures is key to performing successful angle-based surgery, and the image quality produced depends on the clarity of the lens and cornea as well as stability of the anterior chamber. There may be traces of blood clouding the surface of the gonioscopy lens or obscuring the interface between the lens and the cornea. If this occurs, use balanced salt solution (BSS) to flush the lens and cornea, and then reapply the coupling agent and the gonioscopy lens.
It is also important for the surgeon to be mindful of the pressure being applied, as excessive pressure can cause corneal folds or cause viscoelastic egress, distorting the image. Taking a moment to lighten up on the pressure or the refill the anterior chamber may help improve the image.
Sometimes the patient may need to move their eye to look further nasally to optimize visualization of the angle. The trabecular meshwork (TM) is a very helpful landmark during angle surgery, and the TM can often be identified by the patient’s natural pigmentation or a red blood-tinged hue from the relative hypotony that results after phacoemulsification. If the TM remains difficult to identify, Trypan blue, used commonly in anterior segment surgeries, can be used to safely stain the TM for identification.6

Figure 5. In this patient undergoing selective laser trabeculoplasty, the narrow angle (A) obscures landmarks and makes visualization difficult. Instructing the patient to look in the direction of the gonioscope mirror (inferiorly in this case) opens the view (B) to the superior angle, clearly revealing the trabecular meshwork and scleral spur.
Gonioscopy Pearls
Although the principles and techniques of gonioscopy are well established, their practical application often varies depending on the clinical scenario. Subtle differences in patient anatomy, pathology, or surgical context can present unique challenges that require adaptation and experience. The following cases illustrate how thoughtful use of gonioscopy—combined with careful technique and problem-solving—can enhance both diagnostic accuracy and surgical outcomes.
Case 1: Selective Laser Trabeculoplasty (SLT) in a Narrow Angle
Treatment of open-angle glaucoma with SLT can be challenging in a case with a relatively narrow angle (not angle closure) or in cases of mixed mechanism glaucoma. There are several methods to facilitate more optimal viewing in these cases.
- Pretreatment with pilocarpine: constricting the pupil with pilocarpine prior to SLT can help with angle viewing in more narrow angles by flattening the peripheral iris and pulling it away from the angle.
- Consensual pupil response: if pilocarpine is not available or was not used, shining a light in the fellow eye can constrict the pupil in both eyes and help open the angle.
- “Looking over the hill” (Figure 5): In the first gonioscope photo, the angle is not visible due to narrow angle. When the patient is instructed to look in the direction of the gonio mirror, the angle rotates and allows the surgeon to “look over the hill” of the iris.

Figure 6. Blood in Schlemm’s canal, viewed here with a direct surgical goniolens, which can be induced by applying peripheral pressure with a large-diameter gonioscopy lens.
Case 2: Diagnostic Use of Compression (Dynamic) Gonioscopy
As previously noted, the type of gonio lens and the size of the area in contact with the surface of the eye dictate what type of forces it places inside the eye. This in turn affects what the lens can do, especially with compression. The smaller diameter 4-mirror lenses press on the central cornea and displace aqueous into the peripheral anterior chamber angle, thus opening a closed angle. This allows for the differentiation of appositional angle closure and synechial angle closure, as the former will open with compression and the latter will not. Conversely, larger diameter lenses press on the sclera peripheral to the limbus, which tends to force blood into Schlemm’s canal (Figure 6). This technique can be used to verify the communication of Schlemm’s canal with the episcleral venous plexus, an important determinant of the successful outcome of angle-based glaucoma surgery such as goniotomy or trabecular stent.
A 66-year-old Caucasian female with severe primary open-angle glaucoma presented with a history of recurrent iridocyclitis treated with topical steroids. The intraocular pressure was elevated on maximal topical medical therapy. With a history of prior failed trabeculectomy, the patient was sent by the uveitis service for consideration of further surgery. On gonioscopic exam, there appeared to be a small amount of blood in the inferior angle. This prompted a careful evaluation for a source of the bleeding. Switching to a larger-diameter 3-mirror gonio lens, peripheral compression was performed, which induced a trickle of blood to flow from a small abnormal vessel that was in the previous sclerotomy and scleral flap area of the trabeculectomy.
The same lens was used to apply argon laser to the sclerotomy area, and the blood vessel was successfully cauterized. This stopped the bleeding, and the topical steroids were discontinued. As a result, the intraocular pressure decreased to the point where it was controlled on topical medications and surgery was avoided.
Case 3: Surgical Treatment of Cyclodialysis Cleft with Endoscopic Angle Evaluation

Figure 7. Intraoperative endoscopic view of the angle and a traumatic cyclodialysis cleft (A) and the same angle after surgical closure using indirect cyclopexy (B).
The patient is a 42-year-old Caucasian male who suffered blunt trauma to the right eye with a tennis ball. After the hyphema cleared, the patient had hypotony with decreased vision to 20/400 level and choroidal folds. Gonioscopy in the clinic revealed a cyclodialysis cleft but it was difficult to visualize the full extent of it due to the hypotony. The decision was made to perform a cyclodialysis repair with intraoperative evaluation of the angle to determine how many clock hours were involved.
During surgery, the ophthalmic endoscope (Endooptiks; BVI) was used to visualize the extent of the cleft (3 clock hours) after the anterior chamber was filled with viscoelastic (Figure 7A). This helped the surgical decision making of placing 2 mattress sutures of 10-0 prolene passing from the sclera through the peripheral iris. The endoscope was again employed to view the repair to ensure that there was no longer any opening of the cleft that could allow significant aqueous drainage (Figure 7B). The intraocular pressure rose to physiologic levels in the low to high teens and the patient recovered their vision of 20/25.
Semiautomated Gonioscopic Imaging System

Figure 8. Nidek GS-1 semiautomated gonioscopic imaging system.
The Nidek GS-1, made by Japanese manufacturer Nidek, is a novel semiautomated gonioscopic imaging system designed to capture high-quality 360° images of the anterior chamber angle in under 1 minute (Figure 8).7 Standard slit-lamp gonioscopic photography is limited, typically capturing only 4 quadrant views and can vary from lighting and operator technique. The GS-1 system addresses these challenges by incorporating a 16-mirror, machine-assisted gonioscopic lens and an automated imaging process that standardizes capture conditions and provides comprehensive angle visualization.7
In a cross-sectional study of 84 eyes (both normal and glaucomatous) from 50 participants, the device successfully imaged the full iridocorneal angle, with imaging completed in less than 60 seconds per eye.7 Imaging was achieved in 96.27% of normal participants and 96.67% of glaucoma patients. To facilitate clinical interpretation and longitudinal comparison, GS-1 produced images in 16-section, circular, and linear formats. A wide spectrum of angle presentations was captured, ranging from narrow/closed to fully open. The device reliably documented postsurgical anatomy and implanted devices such as iStent (Glaukos) and Baerveldt shunts (Johnson and Johnson Vision; Figure 9). Advantages included speed, ease of use by trained technicians, and standardized reproducibility across visits. Limitations included the lack of dynamic (indentation) gonioscopy and reliance on 2-dimensional imaging, which may not provide adequate depth for accurate grading without adjacent context.

Figure 9. Postoperative high-resolution image of a Baerveldt tube shunt captured by the NIDEK GS-1 semiautomated gonioscopic imaging system.
Conclusion
From patient evaluation to treatment, gonioscopy remains an indispensable diagnostic and surgical tool for ophthalmologists. A wide variety of gonioscopy lenses enable visualization of the anterior chamber angle both in the clinic and the operating room, each offering unique advantages depending on the clinical context. Newer modalities—such as endoscopic evaluation during surgery and automated gonioscopic imaging in the clinic—have also emerged as useful alternatives. Mastering gonioscopy technique, including proper setup, patient positioning, and troubleshooting visualization challenges, is essential for accuracy, surgical success, and patient safety. As MIGS and other angle-based procedures become increasingly common, the consistent and thoughtful application of gonioscopy will be more important than ever in delivering high-quality patient care. GP



References
1. Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern. Ophthalmology. 2021;128(1):P71-P150. doi:10.1016/j.ophtha.2020.10.022
2. Coleman AL, Yu F, Evans SJ. Use of gonioscopy in Medicare beneficiaries before glaucoma surgery. J Glaucoma. 2006;15(6):486-493. doi:10.1097/01.IJG.0000212287.62798.8F
3. Alward WLM, Longmuir RA. Principles of gonioscopy. In: Color Atlas of Gonioscopy. American Academy of Ophthalmology; 2001:9-16. Accessed October 7, 2025. https://www.aao.org/education/disease-review/principles-of-gonioscopy
4. Shareef S, Alward W, Crandall A, Vold S, Ahmed I. Intra-operative gonioscopy: a key to successful angle surgery. Expert Rev Ophthalmol. 2014; 9(6):515-527. doi:10.1586/17469899.2014.973022
5. Kitzmann AS, Fethke NB, Baratz KH, Zimmerman MB, Hackbarth DJ, Gehrs KM. A survey study of musculoskeletal disorders among eye care physicians compared with family medicine physicians. Ophthalmology. 2012;119(2):213-220. doi:10.1016/j.ophtha.2011.06.034
6. Jhanji V, Chan E, Das S, Zhang H, Vajpayee RB. Trypan blue dye for anterior segment surgeries. Eye (Lond). 2011;25(9):1113-1120. doi:10.1038/eye.2011.139
7. Shi Y, Yang X, Marion KM, Francis BA, Sadda SR, Chopra V. Novel and semiautomated 360° gonioscopic anterior chamber angle imaging in under 60 seconds. Ophthalmol Glaucoma. 2019;2(4):215-223. doi:10.1016/j.ogla.2019.04.002