







Despite advances in glaucoma management, intraocular pressure (IOP) remains the only modifiable risk factor for disease progression. As a result, in-office IOP measurements continue to guide clinical and surgical decision-making. Pressure readings are influenced by multiple variables, including corneal pathology, measurement method, examiner expertise, patient comfort, and physiologic variation related to the time of day at which measurements are obtained.1
It is well established that IOP varies throughout the day, even in individuals without glaucoma.2 Patients with glaucoma may experience even greater pressure fluctuations.3 Although diurnal patterns vary among individuals, many patients demonstrate peak IOP during the early morning hours, often while asleep.2,4 Consequently, clinic-based measurements may not accurately reflect a patient’s true IOP profile across the full diurnal cycle. Even Goldmann applanation tonometry (GAT), the gold standard for IOP measurement, provides only a single time-point assessment.

Figure 1. The iCare Home2 is the only home tonometer that is approved for patient self-measurement by the US Food and Drug Administration.
Home tonometry devices have been developed to provide clinicians and patients with a more complete view of IOP trends throughout the day, allowing improved detection of pressure fluctuations and peaks. In the United States, the most widely available home tonometry devices are from iCare USA (Figure 1). Both the iCare Home and the newer iCare Home2 model are FDA approved for patient self-measurement. Compared with its predecessor, iCare Home2 offers several advantages, including the ability to measure IOP in the supine position and integration with a mobile application for data tracking. Patients may rent the device or purchase it through multiple distributors.
Benefits of Home Tonometry
The clinical utility of home tonometry is well recognized. It is particularly valuable in patients who demonstrate structural or functional progression despite IOP readings in clinic that appear to be at target. In such cases, identifying peak pressures or excessive diurnal fluctuation can inform subsequent management decisions. In one study using iCare Home tonometry, up to one-third of patients were found to have peak IOP measurements outside of clinic hours.4 Home monitoring can help distinguish patients whose peak pressures are missed during office visits from those whose progression may be relatively pressure independent, prompting evaluation for additional risk factors for optic neuropathy.
Home tonometry is also useful for assessing the impact of therapeutic interventions before changes become apparent on structural or functional testing. When baseline IOP is within the normal range, the effectiveness of an intervention may not be evident for months or years. This is particularly relevant for therapies such as topical medications, selective laser trabeculoplasty, and minimally invasive glaucoma procedures, which may act in part by blunting IOP spikes rather than lowering mean pressure. Comparing iCare Home measurements before and after a treatment change can provide objective evidence of IOP reduction or reduced fluctuation, offering reassurance to both patient and clinician. Conversely, identifying persistent peaks or variability may allow earlier intervention, before progression is detected on testing.
An additional benefit of home tonometry is increased patient engagement. In our experience, patients using iCare Home often take a more active role in their care, monitoring pressures in relation to medication use, lifestyle factors, or perceived triggers. Similar to findings in hypertension, where home blood pressure monitoring is associated with improved medication adherence,5 home IOP monitoring may promote greater involvement and compliance among patients with glaucoma.
Overall, IOP measurements obtained with the iCare Home device show good agreement with GAT. A recent systematic review found strong correlation between the 2 methods across most studies.1 However, some studies have reported that iCare Home may underestimate IOP at lower pressure ranges and overestimate IOP at higher ranges compared with GAT.6-7 Central corneal thickness may contribute to these differences, with greater discrepancies observed in eyes with thicker corneas.
Limitations of Home Tonometry
Despite its potential benefits, home tonometry may not be appropriate for all patients. Cost remains a significant barrier. Although renting the device may be more affordable than purchasing it outright, the expense can still be prohibitive. At present, home tonometry devices are not covered by Medicare or most commercial insurers. Some insurance plans may reimburse patients for rental or purchase costs if claims are submitted, and certain vendors, such as myeyes.net, assist patients with the reimbursement process. Health savings account (HSA) and flexible spending account (FSA) funds may also be used. Even with these options, cost remains a deterrent for many patients
Home tonometry also requires the dexterity to physically manipulate the device so accurate measurements are obtained. Although the device is generally easy to use, some patients are unable to operate it because of motor or rheumatologic limitations, such as tremors, advanced arthritis, or joint contractures. Others may require additional instruction beyond online training materials. For example, a patient at our institution who rented an iCare Home2 device was unable to use it for 2 weeks because she could not learn the technique from videos alone and required an in-office training visit, necessitating an extension of the rental period. Another patient who purchased the device without a prior trial became frustrated by repeated poor-quality measurements and ultimately regretted the purchase.
Finally, for some patients, the ability to obtain frequent measurements may feel overwhelming, increasing their anxiety. Although many patients find reassurance in home monitoring and feel more engaged in their care, others may experience heightened concern, particularly when recorded pressures are higher than expected. In these cases, counseling and ongoing reassurance may be necessary to support appropriate use of home tonometry.
Alternatives to Home Tonometry
For patients who are unable to perform home tonometry, one alternative is the water drinking test, which can provide a good in-office estimate of peak IOP. In a recently published study, peak IOP during the water drinking test was found to correlate strongly with peak IOP measured with the iCare Home.8 The test is performed by first measuring a baseline IOP, then having the patient drink a large volume of water (typically a liter) in 5 minutes. The IOP is then measured 3 or 4 times at 15-minute intervals over the course of an hour. The highest value obtained is assumed to represent the patient’s peak pressure.
Although the underlying physiology is not fully understood, the test is thought to function as a stress test, or “water challenge,” to the eye’s outflow facility. For clinics or patients unable to accommodate prolonged visits, alternating between early morning and afternoon appointments may offer insight into an individual patient’s diurnal IOP fluctuation patterns.
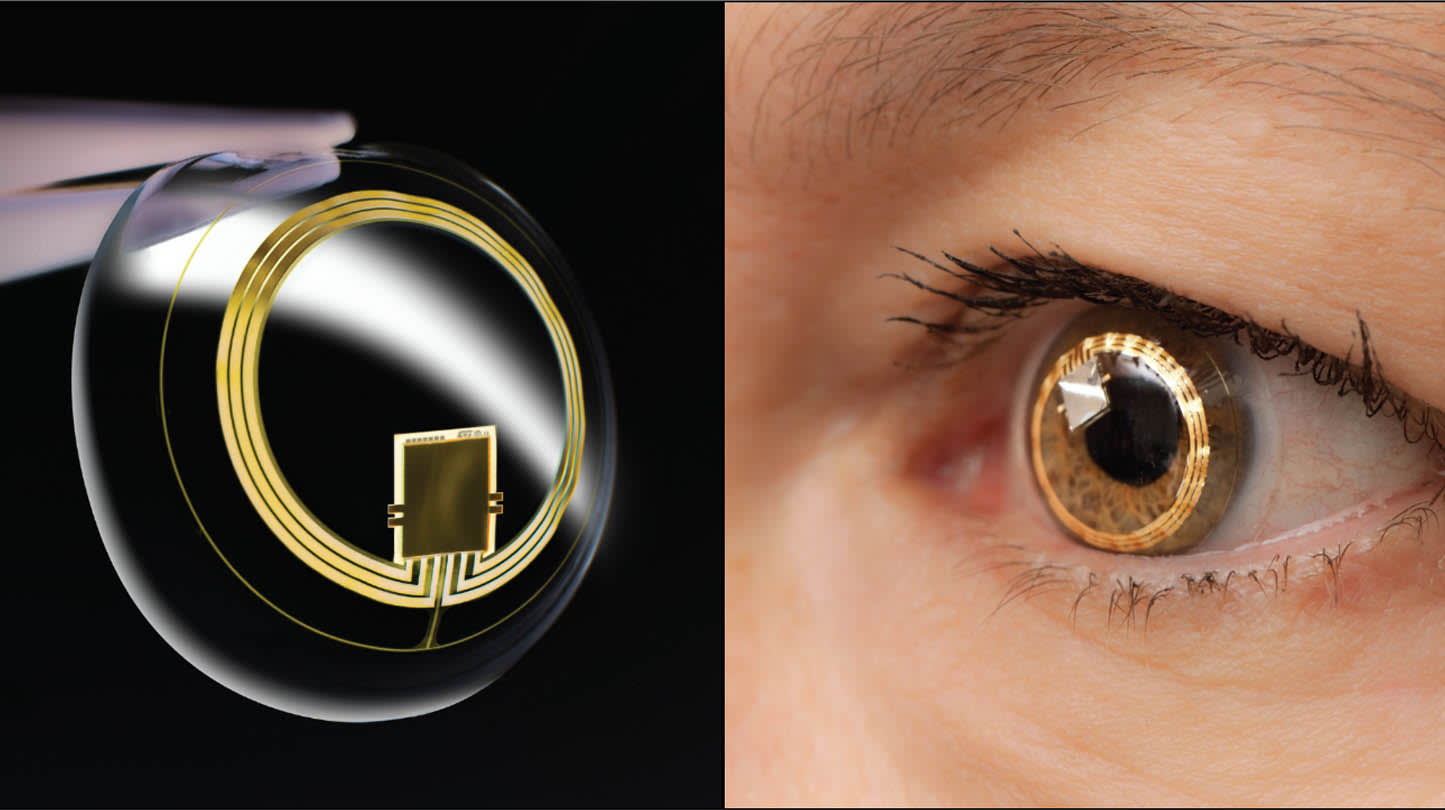
Figure 2. The Triggerfish contact lens sensor (Sensimed) is a soft, wireless contact lens that continuously monitors intraocular pressure (IOP)–related ocular dimensional changes over 24 hours. The sensor detects subtle corneal shape fluctuations caused by IOP variations and transmits the data to an external recorder for analysis of circadian pressure patterns.
Continuous Home Tonometry
Although more informative than a single in-office measurement, self-monitoring IOP with a device such as the iCare Home still provides only snapshots in time. Continuous ocular tonometry could provide a more comprehensive understanding of IOP behavior, including fluctuations that occur outside scheduled measurement times.
The Triggerfish contact lens sensor (Sensimed) is an FDA-approved device that measures relative changes in ocular pressure throughout the day (Figure 2). A key limitation, however, is that it does not measure absolute IOP values. As a result, it can demonstrate trends over time but does not provide true IOP measurements.9 Currently, its use is largely limited to research settings.
The Eyemate-IO (Implandata) is another technology under investigation. This foldable sensor is implanted in the ciliary sulcus at the time of cataract surgery and allows for continuous IOP measurement.10 Notably, it provides cornea-independent pressure readings. In a recent study of 8 patients with primary open-angle glaucoma who underwent cataract surgery with Eyemate-IO implantation, higher mean IOP, higher peak IOP, and greater IOP fluctuations were significantly associated with faster retinal nerve fiber layer thinning.10 Although larger studies are needed, Eyemate-IO represents a promising direction for future glaucoma management.
Conclusion
As with any glaucoma intervention, recommendations for home tonometry should be guided by clinical judgment, with careful consideration of the potential benefits and burdens for each patient. The best candidates are typically those who continue to progress despite seemingly adequate IOP control. Home tonometry may also help assess the effectiveness of glaucoma interventions before changes become apparent on traditional testing and can encourage greater patient engagement in care.
Even when devices and training are provided through third parties, clinicians must be available to support patients throughout the process as needed. As with all additional data, home tonometry measurements must be interpreted within the broader clinical picture. Despite its current limitations, home tonometry represents an increasingly valuable tool for both patients and providers. GP


References
1. Pons-Talaya C, Pons-Talaya A, Widmer J, et al. Effectiveness and accuracy of iCare Home tonometer in glaucoma patients: a systematic review. Am J Ophthalmol. 2026;282:69-81. doi:10.1016/j.ajo.2025.10.008
2. Asrani SG, McGlumphy EJ, Al-Aswad LA, et al. The relationship between intraocular pressure and glaucoma: an evolving concept. Prog Retin Eye Res. 2024;103:101303. doi:10.1016/j.preteyeres.2024.101303
3. Tojo N, Abe S, Ishida M, Yagou T, Hayashi A. The fluctuation of intraocular pressure measured by a contact lens sensor in normal-tension glaucoma patients and nonglaucoma subjects. J Glaucoma. 2017;26(3):195-200. doi:10.1097/IJG.0000000000000517
4. Perkins SW, Joo JH, Allan KC, et al. Home tonometry diurnal intraocular pressure patterns, patient adherence, and measurement reliability in a prospective clinical cohort. Clin Ophthalmol. 2025;19:3547-3556. doi:10.2147/OPTH.S545165
5. Fletcher BR, Hartmann-Boyce J, Hinton L, McManus RJ. The effect of self-monitoring of blood pressure on medication adherence and lifestyle factors: a systematic review and meta-analysis. Am J Hypertens. 2015;28(10):1209-1221. doi:10.1093/ajh/hpv008
6. Kratz A, Zbidat R, Kishner R, Cohen M, Shalata W, Goldberg I. Assessment of the iCare HOME2, a new intraocular pressure self-measurement tonometer. J Glaucoma. 2023;32(11):926-929. doi:10.1097/IJG.0000000000002298
7. Liu J, De Francesco T, Schlenker M, Ahmed II. iCare Home tonometer: a review of characteristics and clinical utility. Clin Ophthalmol. 2020;14:4031-4045. doi:10.2147/OPTH.S284844.
8. Susanna CN, Susanna FN, Cyrino LG, et al. Agreement between the iCare Home tonometer and the Goldmann applanation tonometer in the assessment of the peak intraocular pressure in the water-drinking test. Ophthalmol Glaucoma. 2025;8(3):235-241. doi:10.1016/j.ogla.2024.11.008
9. Sunaric-Megevand G, Leuenberger P, Preußner PR. Assessment of the Triggerfish contact lens sensor for measurement of intraocular pressure variations. Acta Ophthalmol. 2014;92(5):e414-e415. doi:10.1111/aos.12455
10. Micheletti E, Rao H, Weinreb RN, Mansouri K; EYEMATE-IO study group. Intraocular pressure monitoring using an implantable sensor detects structural glaucoma progression in the EYEMATE-IO Trial. Am J Ophthalmol. 2025;277:112-119. doi:10.1016/j.ajo.2025.05.010