For Glaucoma Physician's Surgical Pearls video series, Shivani S. Kamat, MD; Mary Qiu, MD; and Arsham Sheybani, MD, demonstrate several ways to perform a 360° GATT using the iTrack Advance (Nova Eye Medical). Transcript of the narration follows below:
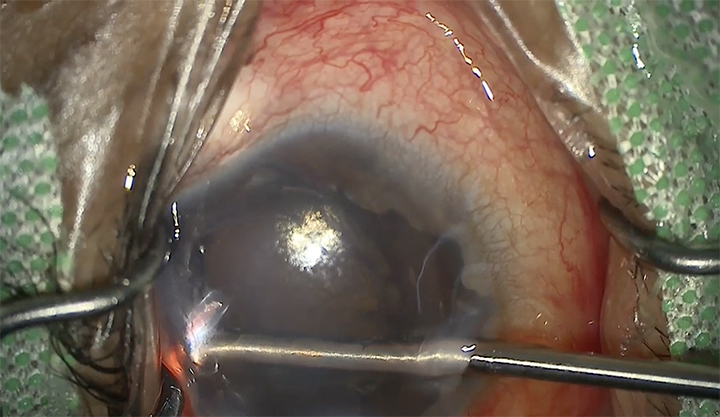
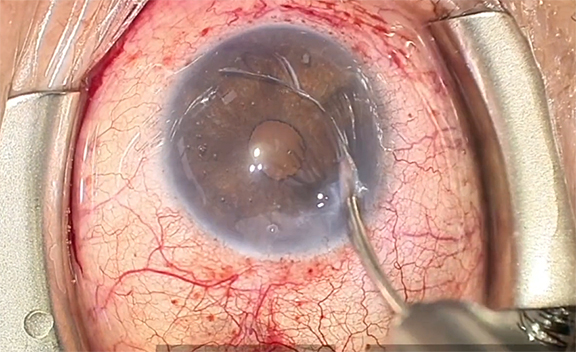
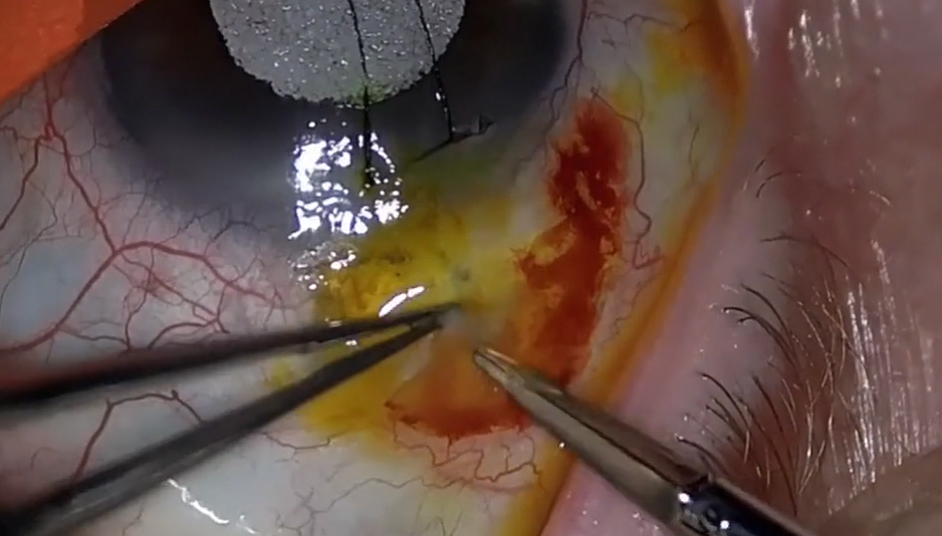
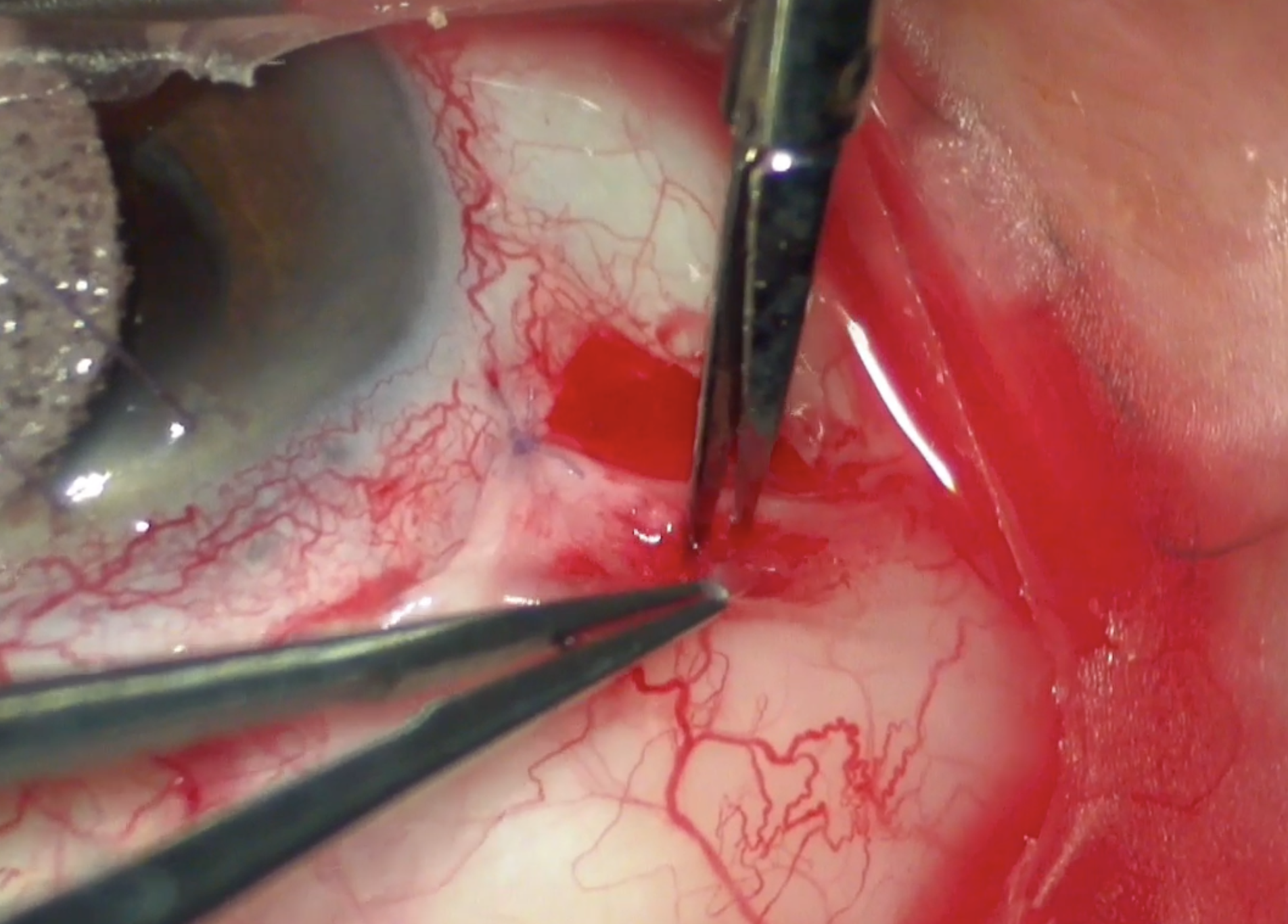
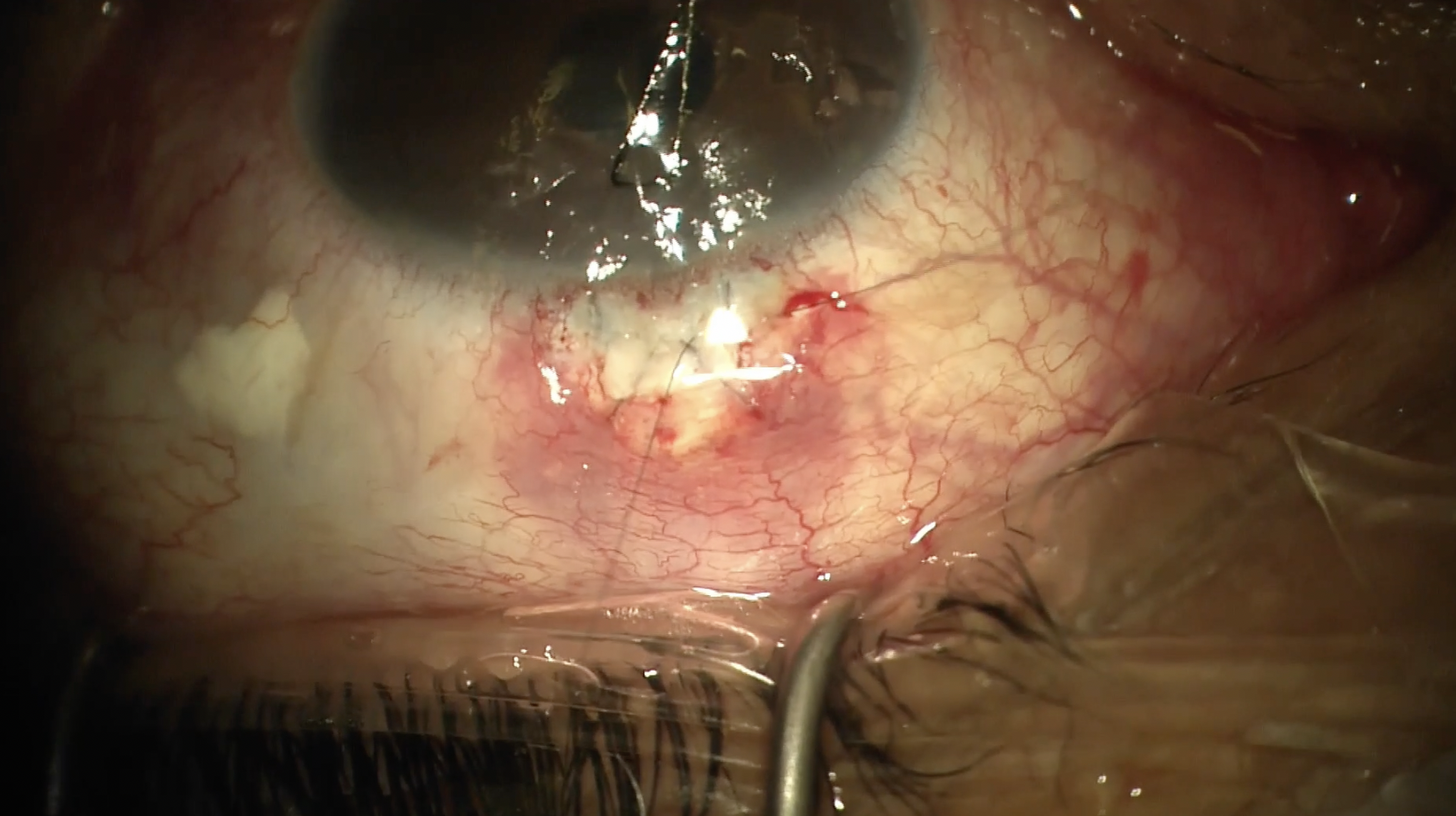
This video demonstrates 3 different ways to do a 360° GATT with an iTrack Advance. This technique demonstrated by Shivani Kamat, MD, does require retrieval of the tip of the catheter and an assistant to hold the prism. The metal tip of the injector is used to make a small otomy and the iTrack catheter is inserted into Schlemm’s canal. The slider is pushed forward to advance the catheter all the way around. The blinking light can be seen coming around the limbus. The assistant clicks the clicker to dispense viscoelastic into Schlemm’s canals to perform a canaloplasty, and some blanching can be seen. Once the catheter comes all the way around, the prism is given to the assistant to hold, and the primary surgeon can use the nondominant hand to use MST forceps to grab the tip of the catheter. The injector is pulled out of the eye to perform a 360° trabeculotomy, and then the forceps can release the tip of the catheter.
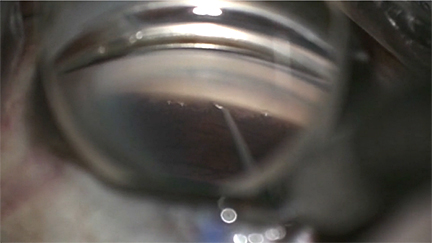
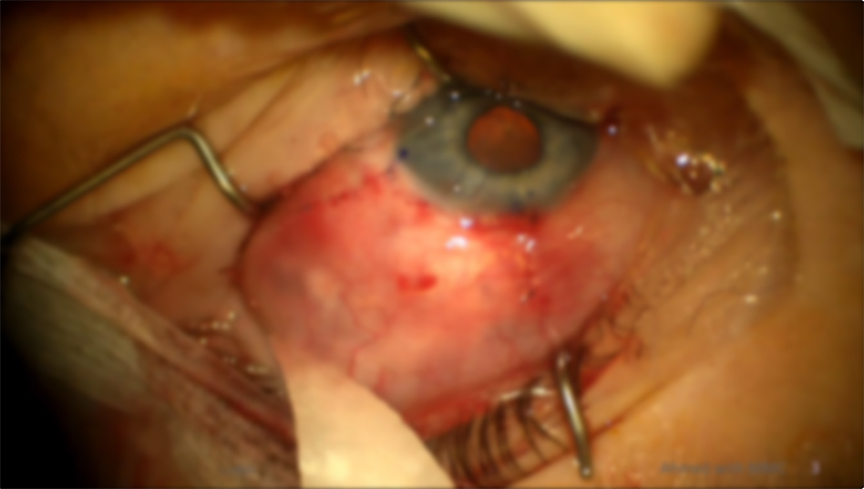
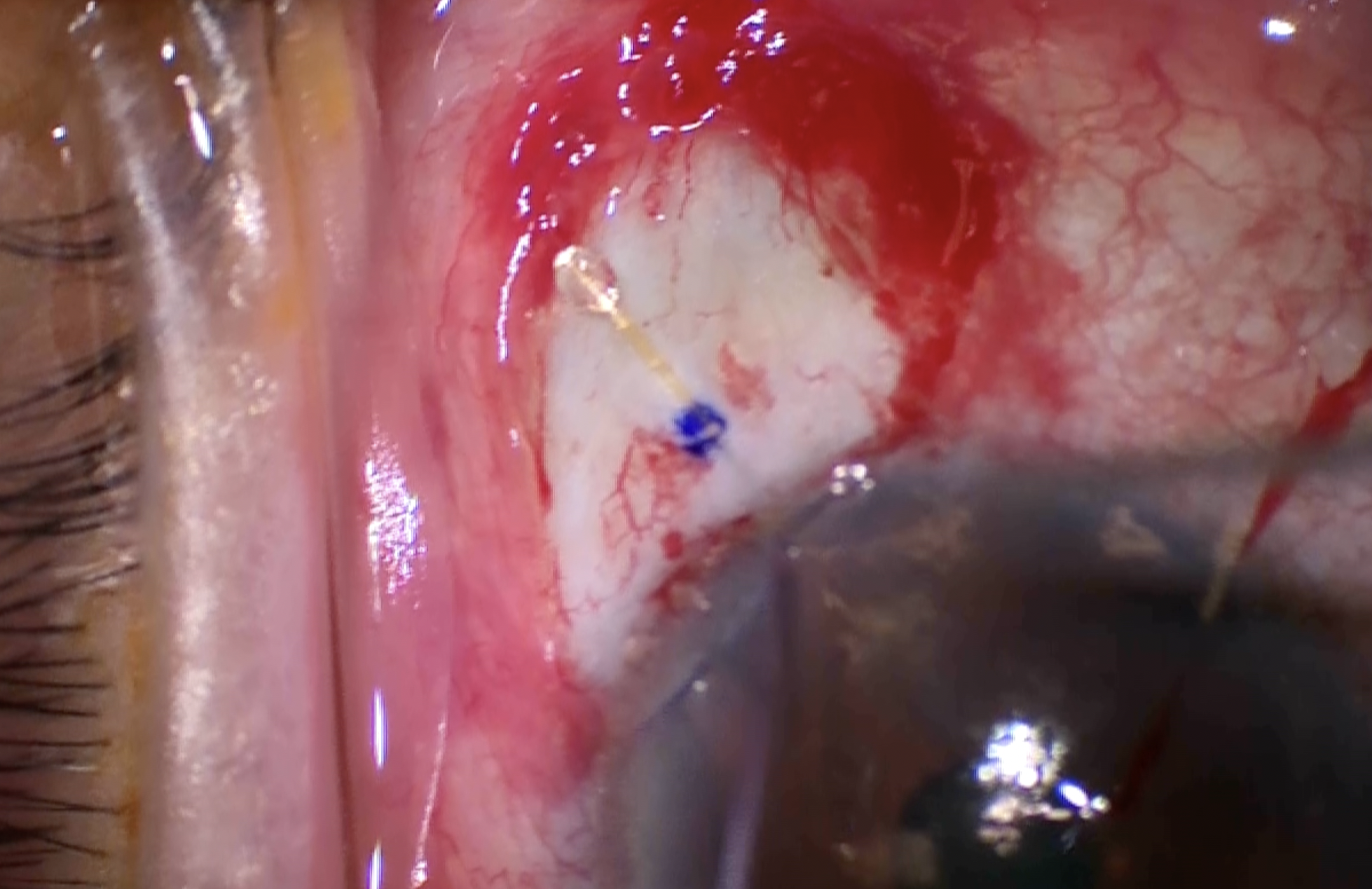
A variation on this technique demonstrated by me, Mary Qiu, MD, and my PGY4 resident Ian Patterson, uses a hands-free prism and does not require an assistant, so the primary surgeon can retrieve the tip of the catheter with the nondominant hand. The view was a bit blurry due to the cornea, so a Grieshaber blade was used to make a short otomy into the nasal TM to better visualize the back wall of Schlemm’s. A Katena hands-free prism was placed onto the surface of the cornea and gently pressed down so it would suction onto the surface of the eye and not slip. The iTrack Advance was inserted into a para, advanced across the AC, seated into Schlemm’s, and the slider was pushed forward to advance the catheter into Schlemm’s. As the catheter comes around, the blinking red light can be seen behind the limbus. The assistant clicks the clicker to dispense viscoelastic into Schlemm’s, performing a canaloplasty. Once the catheter comes all the way around, the blinking red light can be seen to appear in the initial otomy site. MST forceps in the nondominant hand can be inserted into the main wound, advanced across the AC and over or under the iTrack injector, to retrieve the catheter tip. Once the tip of the catheter is grasped with MST forceps, the injector can be pulled out of the eye to perform a 360° trabeculotomy, and the tip of the catheter can be released by the MST forceps.
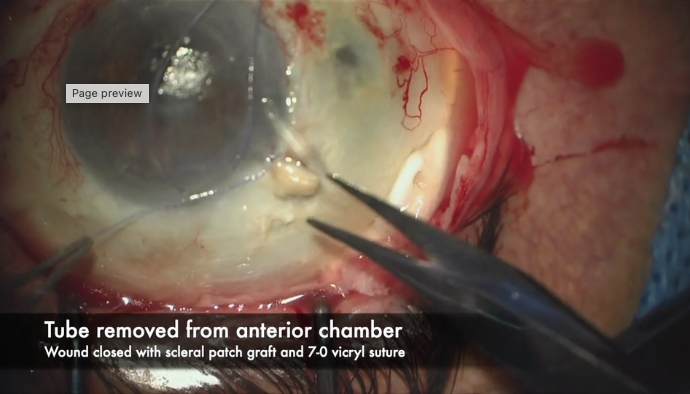
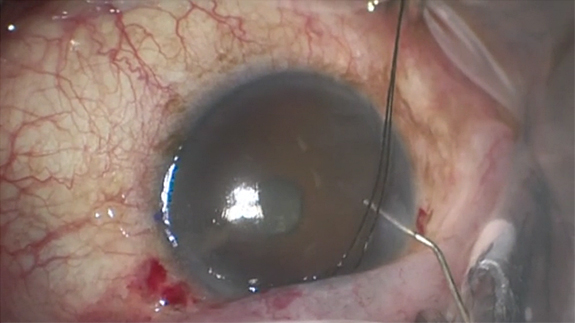
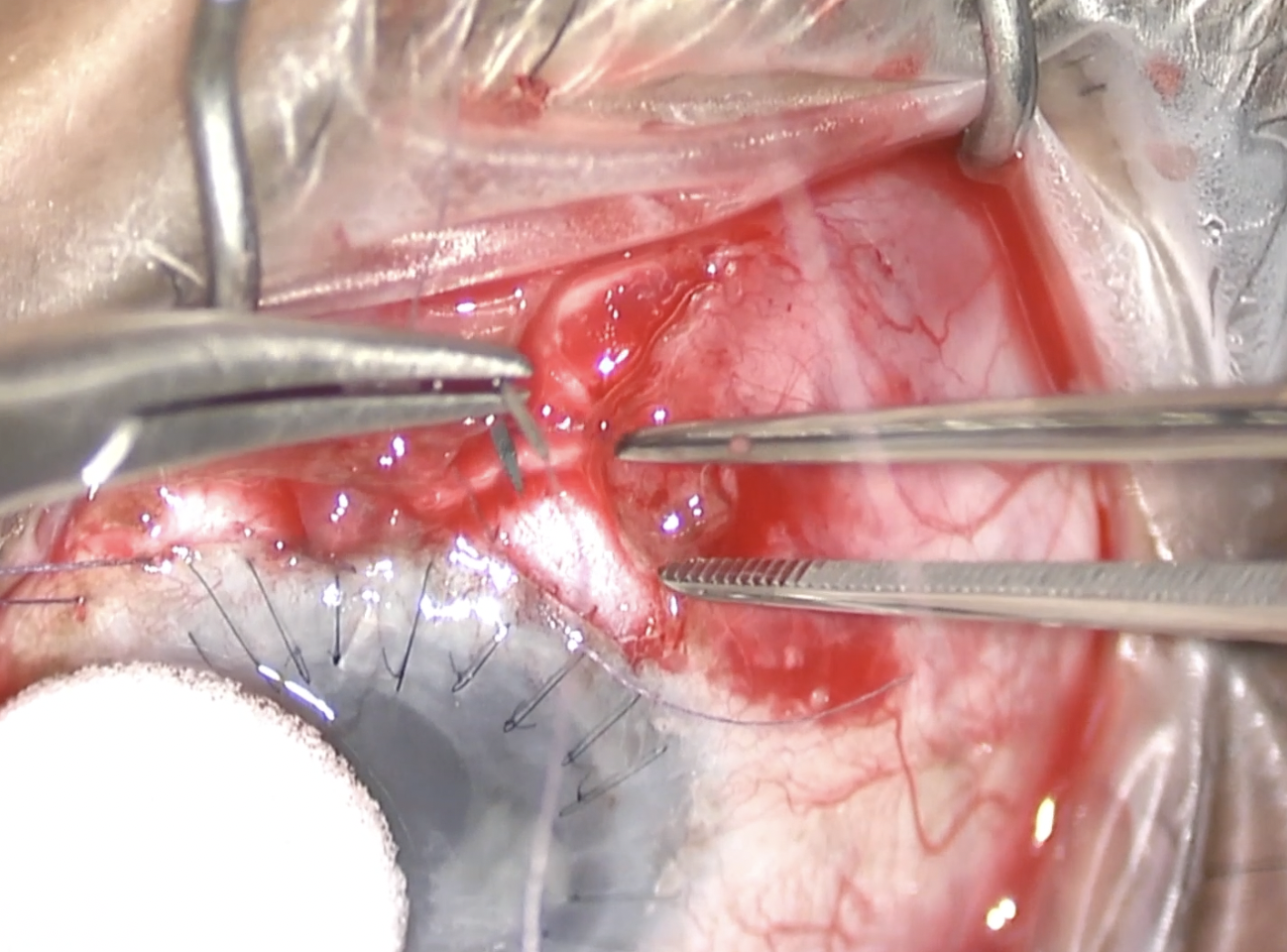
The second technique, demonstrated by me, Mary Qiu, does require the retrieval of the tip of the catheter but does not require an assistant to hold the prism. In this particular case, an otomy has been premade with a Sinskey, but this is not necessary. Again, the injector is seated into Schlemm’s canal, and the slider is pushed forward to advance the catheter all the way around Schlemm’s. The assistant clicks the clicker to dispense viscoelastic, performing a canaloplasty. Dramatic blanching can be seen. Once the catheter has made it all the way around and the blinking light can be seen in the otomy, the injector can be pulled out of the para, and the slider should be pushed forward to keep the catheter in place as the injector is backed out. The catheter can be cut off the injector to free up the dominant hand. If an assistant is available, she can hold this cut end of the catheter with a needle driver to prevent it from falling back into the eye. But if there is no assistant available, the cut end of the catheter can just be left here in this para. With the dominant hand, MST forceps can be used to retrieve the catheter as it appears in the otomy. The prism is removed, and the tail of the catheter can be pulled to perform a GATT in the usual fashion. This technique was inspired by Rupak K. Dhoot, MD, the 2022 glaucoma fellow at the Cole Eye Institute at Cleveland Clinic.
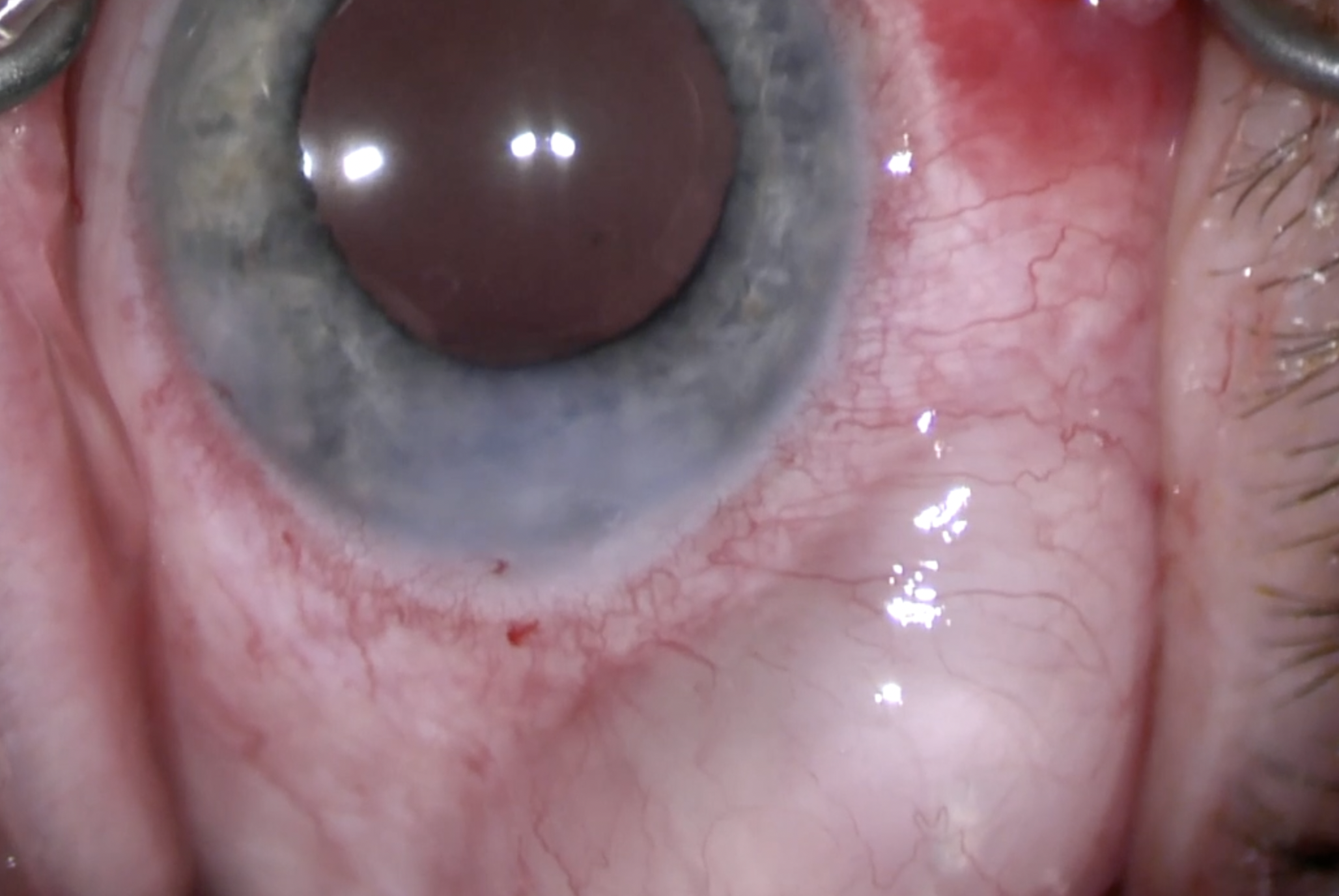
This third technique, demonstrated by Arsham Sheybani, MD, does not require the retrieval of the tip of the catheter or an assistant to hold the prism.
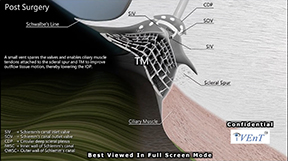
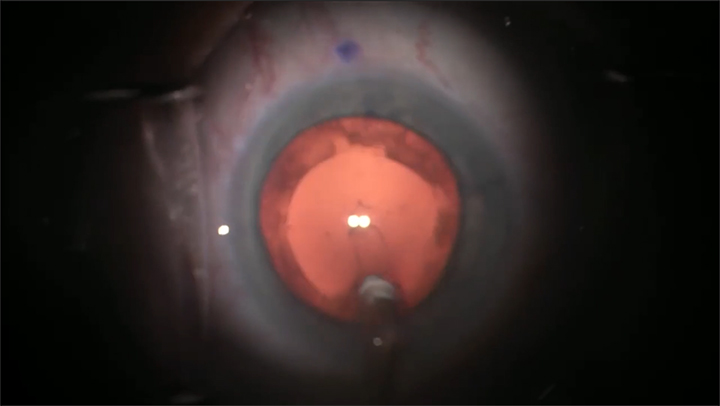
Arsham Sheybani here, describing a technique using the iTrack Advance catheter for performing a 360° ab interno goniotomy, in this case a GATT. What we do is when we thread into the canal and we see the light come back to us, we’re actually going to continue to move the injector into the angle by fulcruming in the wound. We're not advancing the catheter; it's already maximally advanced. Once we get to the tip being about 180° or just past the 180° from the wound that we’re in, after we fulcrum, we’ll then pull back out of the eye, and this helps keep the catheter engaged inside the canal so it doesn’t backtrack or slide out. As you can see, we are not doing anything with the slider. All we did was exit the wound once we were 180° apart from it.
Thank you so much for watching our video. Please e-mail us if you have any questions or comments.

Other Videos From Series