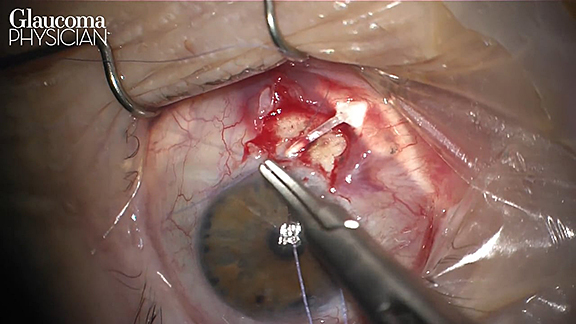
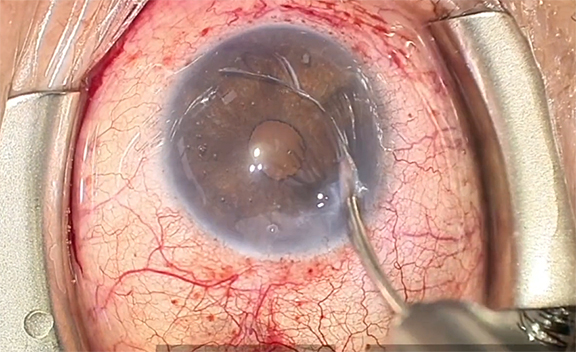
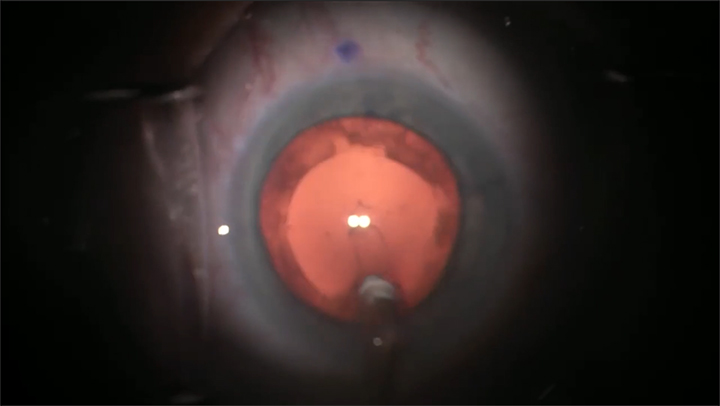
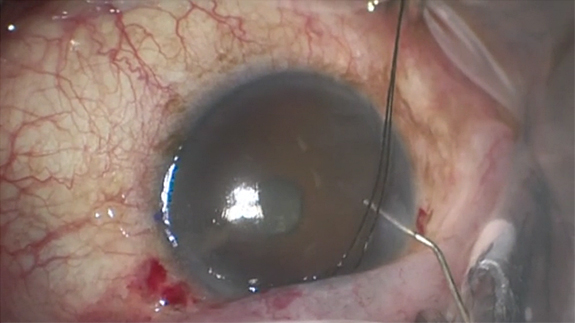
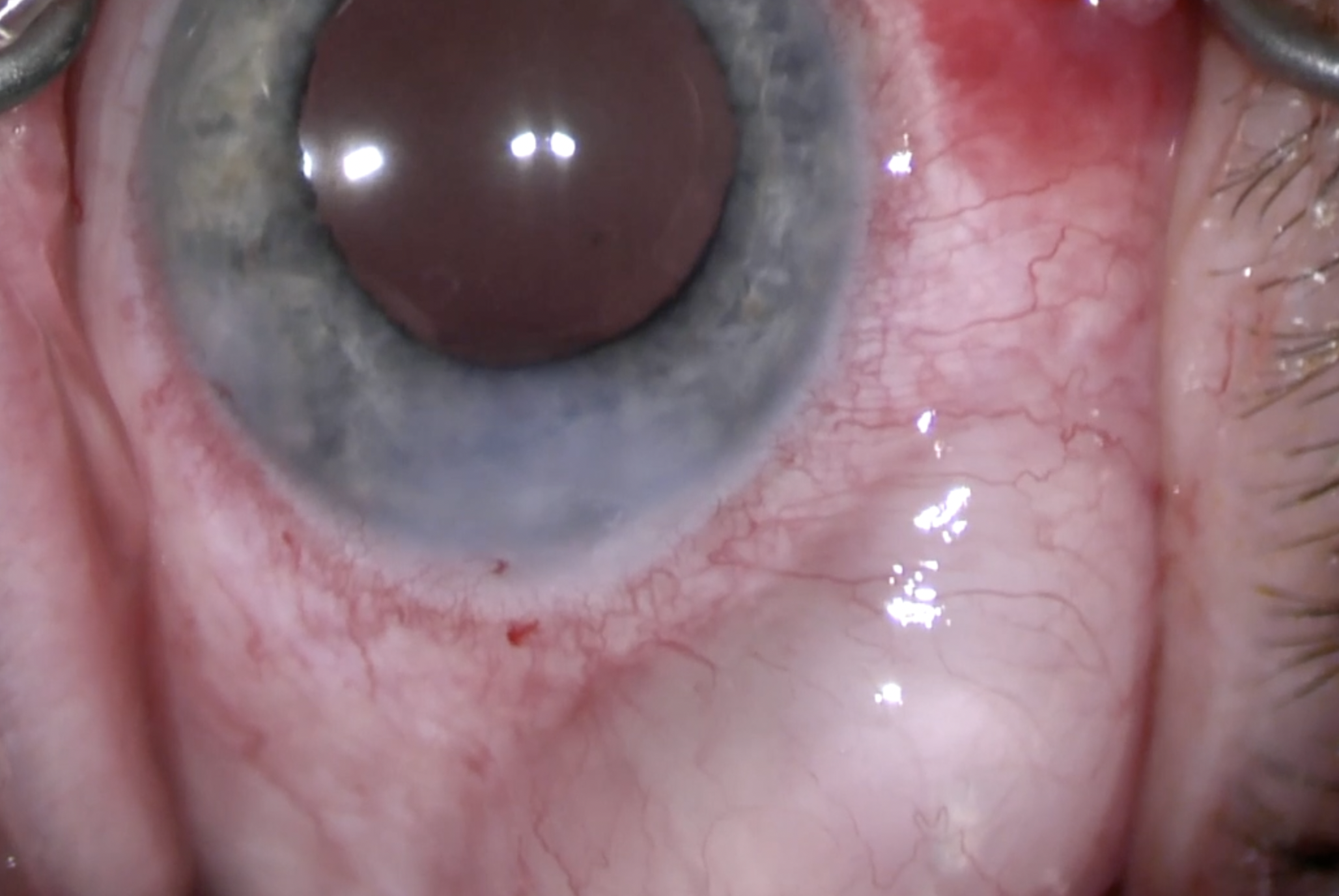
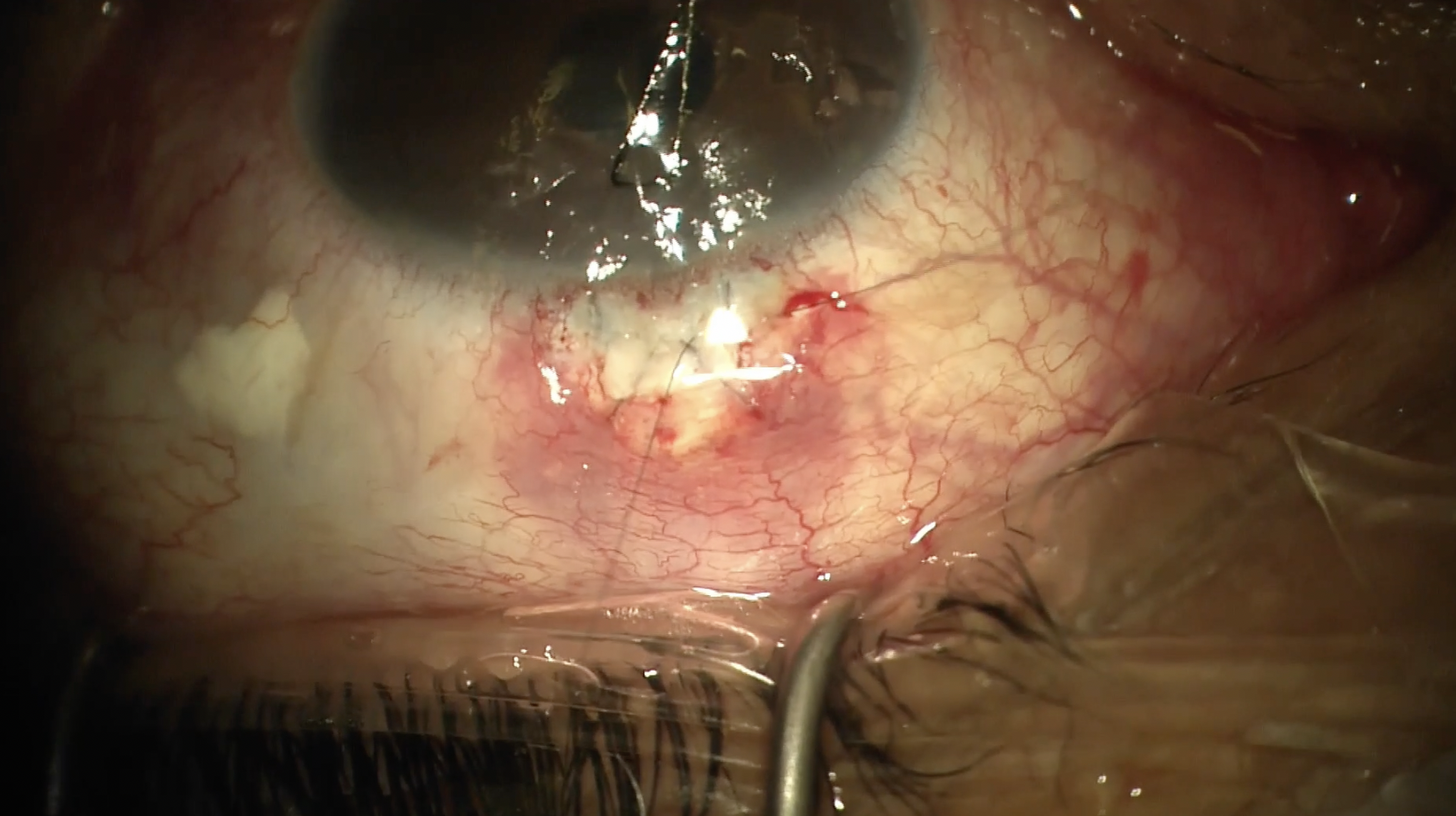
I would like to share an interesting and helpful technique. This patient was referred for an open “conj.” [conjunctiva] Xen [AbbVie] revision. The patient had undergone superiotemporal open conj. ab-externo placement of a Xen. The referring surgeon used 40 μg of mitomycin C and was trying to avoid the preexisting failed “trab” [trabeculectomy] site superionasally. You can see I'm being very gentle here trying to find the right spot to open this scarred adherent conj. The bleb you're looking at right now failed quickly despite an open conj. technique. You can see it's very flat, vascular, and thick. It did respond to ocular compression in the clinic with a mild bleb rise. So, I knew the Xen was patent, but clearly there was too much bleb resistance and it wasn't amenable to needling. I'm being really gentle while opening conj. here because the conj. is pretty friable, and it's very adherent to the underlying Tenon’s [capsule]. You can see just how thick this bleb is. Opening along the limbus, you want be very mindful not to bisect or dislodge the Xen. It can be difficult to see exactly where the Xen is until you have the tissue open. I'm going to dissect a pocket here in the episcleral space. You'll see that there is not a sock of Tenon’s [capsule] around Xen like you have in some situations, but rather just a really thick, unhealthy bleb.
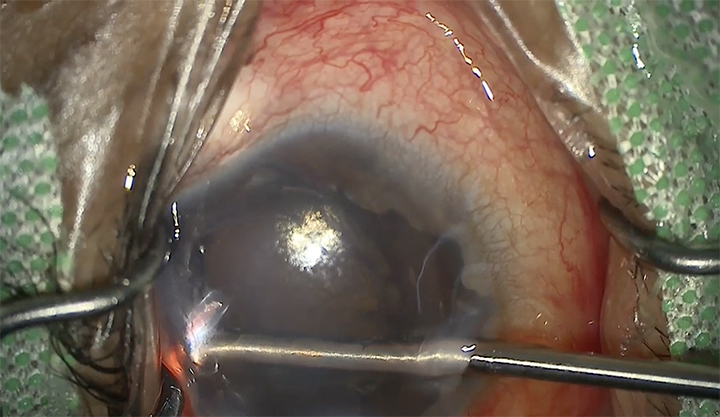
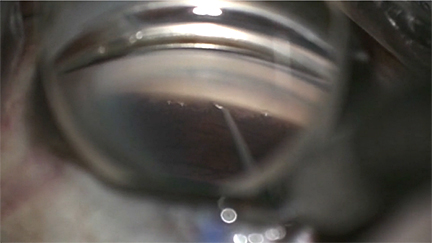
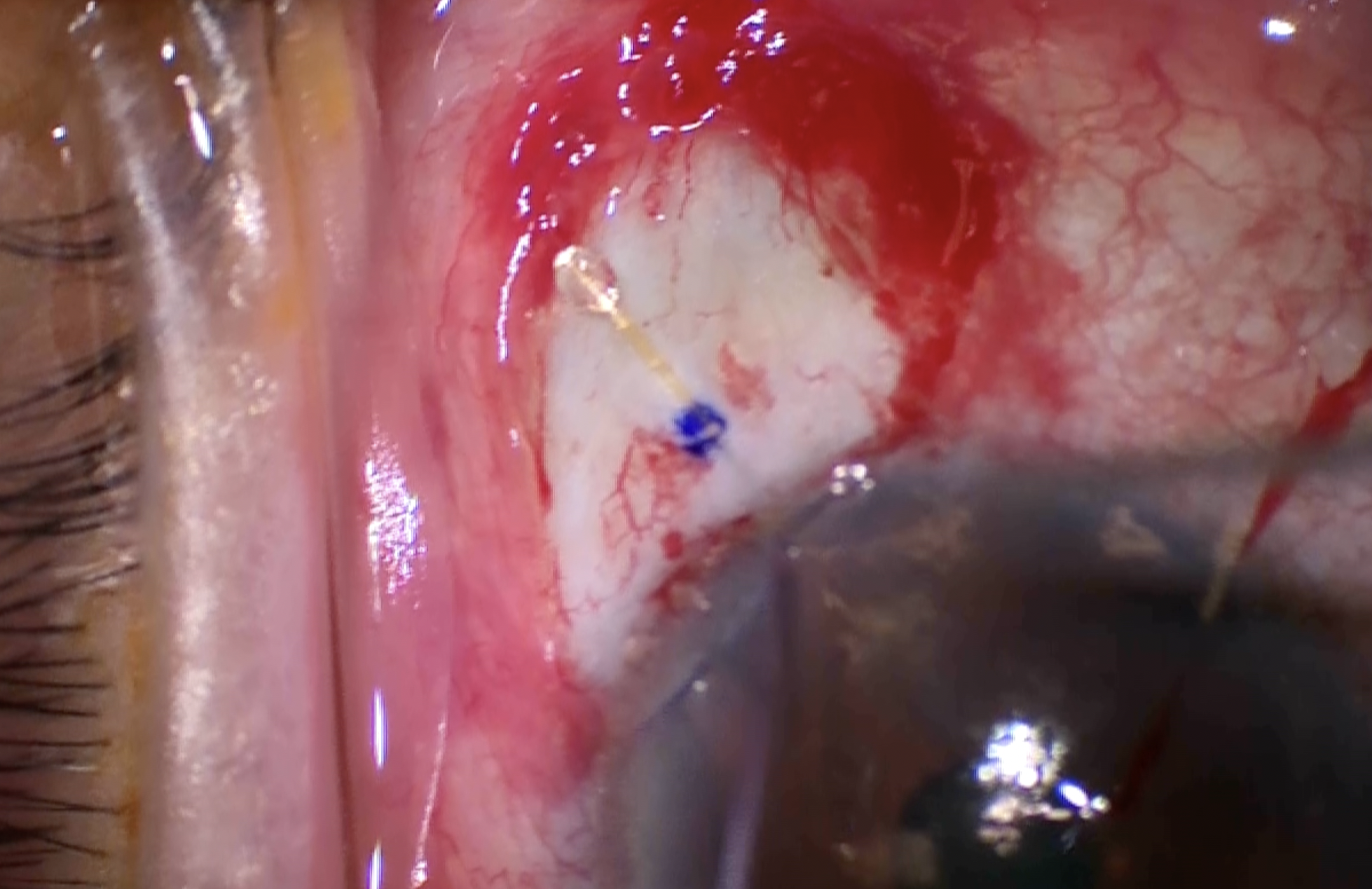
Once I have a nice pocket in that quadrant, I'm just going to confirm that indeed the Xen is flowing. You'll see the little bead of aqueous there at the tip. I start to try and figure out how on Earth, without an assistant, I am going to separate conj. and Tenon’s because I want to remove some of this thick capsule. I don't want to create a buttonhole or leave thin tissue at the limbus. So, what I decide to do is to go ahead and tack that little corner of Tenon’s back just posterior to the limbus where it normally inserts. I'm going to take a strong episcleral bite and engage Tenon’s alone here, and I'll just tie that off with an interrupted suture with 8-0 Vicryl. Now, I have a little Vicryl assistant to help hold Tenon’s while I dissect away conj. I'm being very careful here because I know that conj. by itself is probably pretty thin, and that's confirmed as we go along. You can see just how thin it is. There are areas that are avascular, but once I get back a little more posterior, I feel more confident and can use a Westcott to separate tissue.
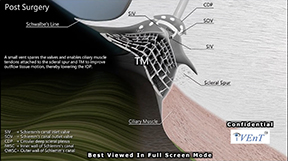
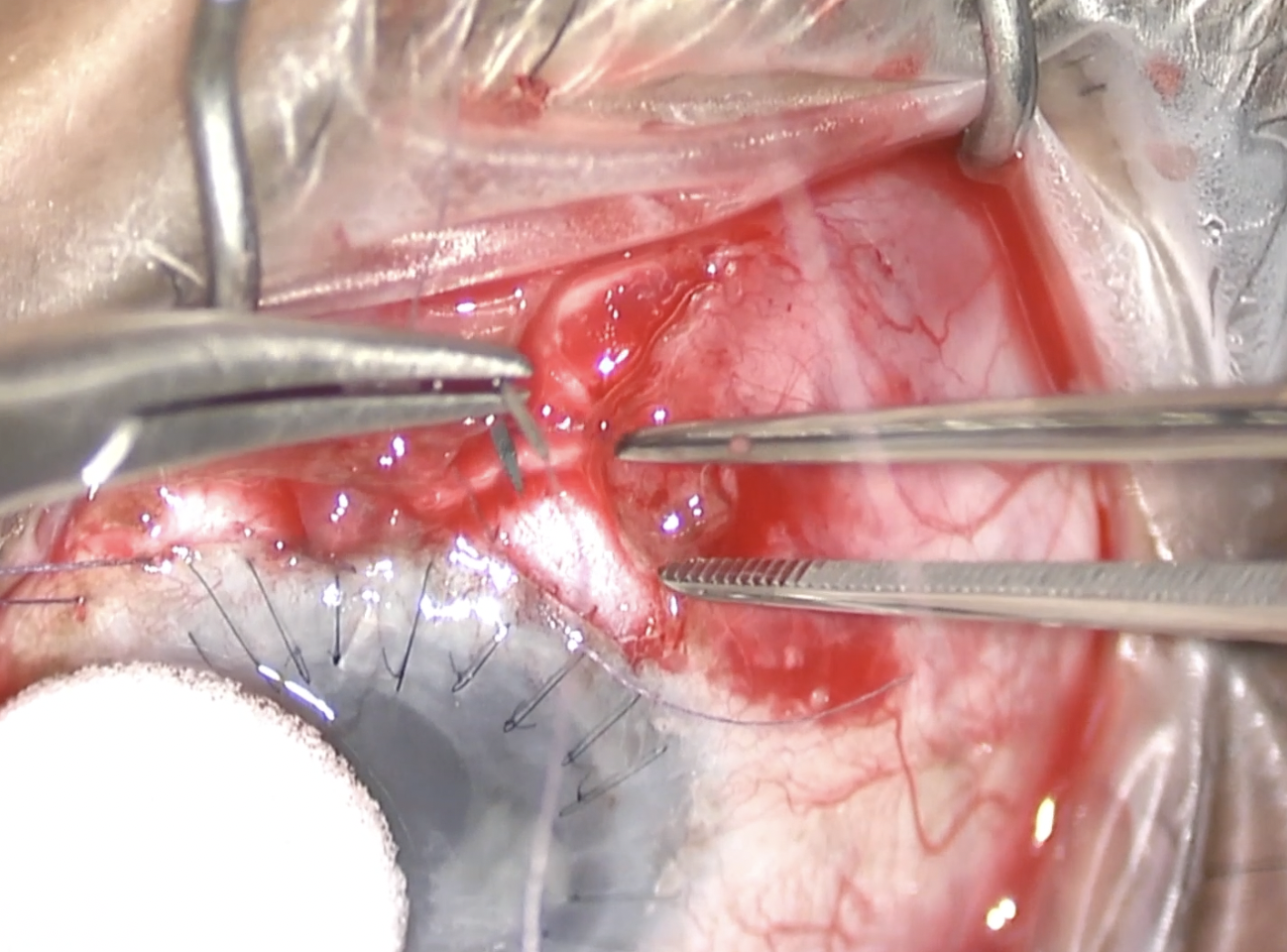
I'm going to tack up the other corner of Tenon’s, and then I'll relax the conj. just so I have a little more exposure. What I'm deciding to do is to make a Tenon’s window and leave a lip of Tenon’s right at the limbus. And I'm hoping this window over the Xen tip will allow for early flow and better long-term filtration with less encapsulation and bleb resistance. To close conj., I'm going to take a bite through the limbus, and then just run it back in a running-locking fashion. Since the conj. is quite scarred there around the “trab,” I'm being really careful to get a nice watertight closure. And then I'll do a similar thing over on the temporal side, running it back, and this time, taking some episcleral bites just to really tack that conj. down in that area that's friable. Checking for a watertight closure, here. Then, what I'm going to do is do a 40 μg injection of mytomycin C, very posterior in an area that's well covered by the eyelid, having cotton tips ready to keep it away from the limbus as it binds. And that's pretty much a wrap. This patient has done really well.

Other Videos From Series