For Glaucoma Physician’s Surgical Pearls video series, Mary Qiu, MD, presents her technique for performing an inferior hemi-GATT using the Via360 surgical system (New World Medical). Transcript of the narration follows below:
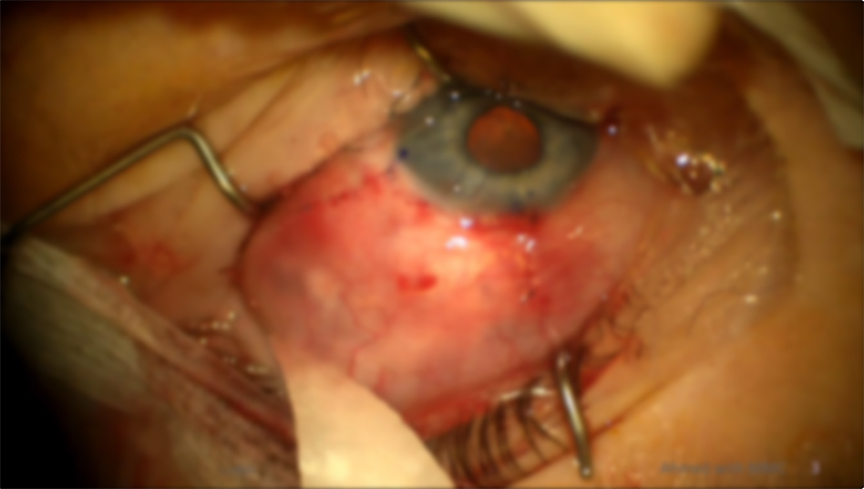
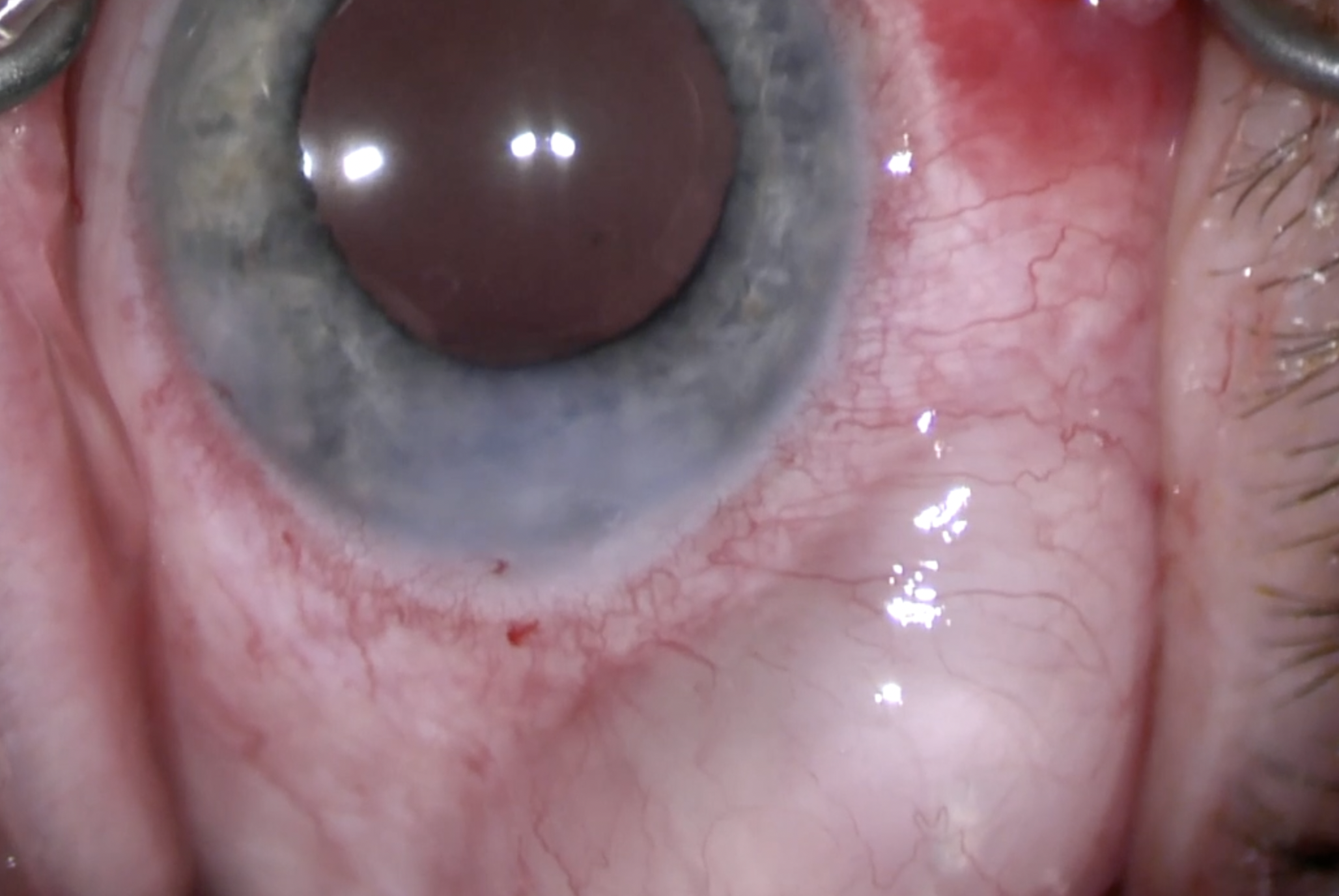
This is a case of a Via360 inferior hemi-GATT in an anticoagulated 75-year-old monocular pseudophakic man with pseudoexfoliation glaucoma and a prior failed trab in his only seeing bright eye.
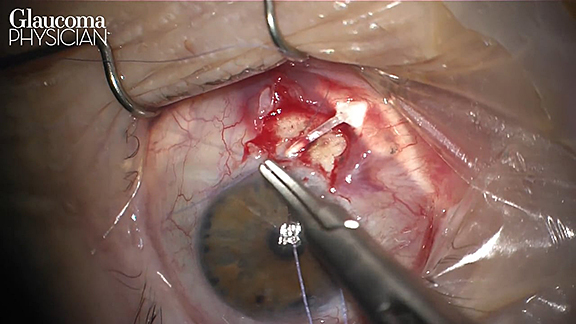
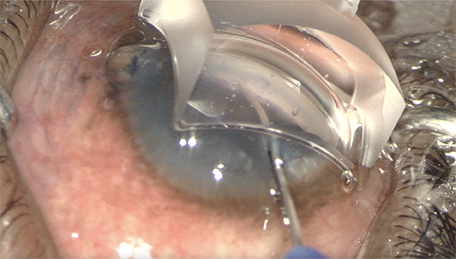
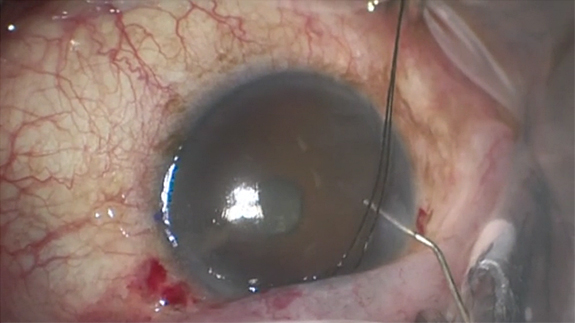
A temporal paracentesis was made and enlarged to at least 1.2 mm to fit the Via360. Lidocaine and miostat were injected into the AC. The AC was filled with Healon5 to tamponade possible reflux bleeding from the angle since he was anticoagulated. A Grieshaber blade was used to make the initial otomy in the nasal angle, though this step could have been done directly with the via360 cannula.
To demonstrate how the handpiece works, the catheter pushes forward when the index finger scrolls forward on the wheel on the handpiece and 3 mL of viscoelastic are dispensed in both the forward and tangential direction when the button on the handpiece is pressed down with the same index finger. The scrolling and the pressing can be done independently.
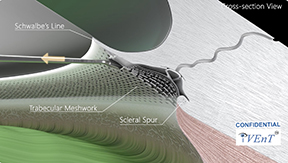
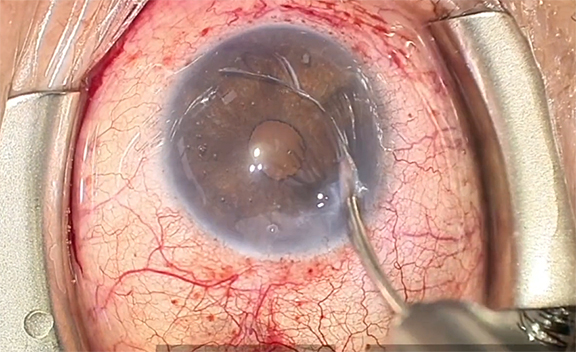
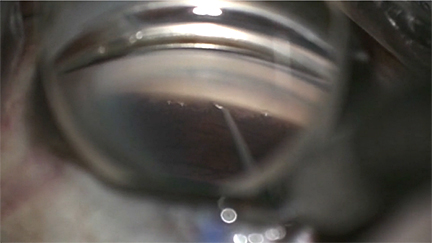
The catheter is scrolled out of the cannula and enters Schlemm's canal. The catheter becomes less visible behind pigmented TM as it continues to move around in a clockwise fashion. On the hand piece, the scroll button is scrolled forward and then the button is pushed down. With every push there’s 3 mL of viscoelastic dispensed. It's not possible to physically see where the tip of the catheter is, so the catheter is advanced carefully—1 scroll and 1 push at a time.
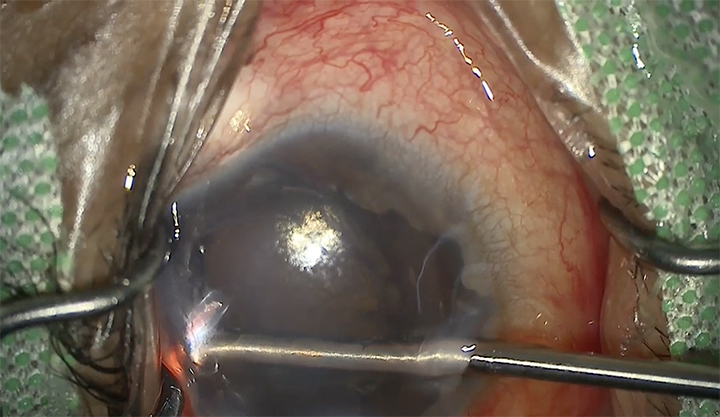
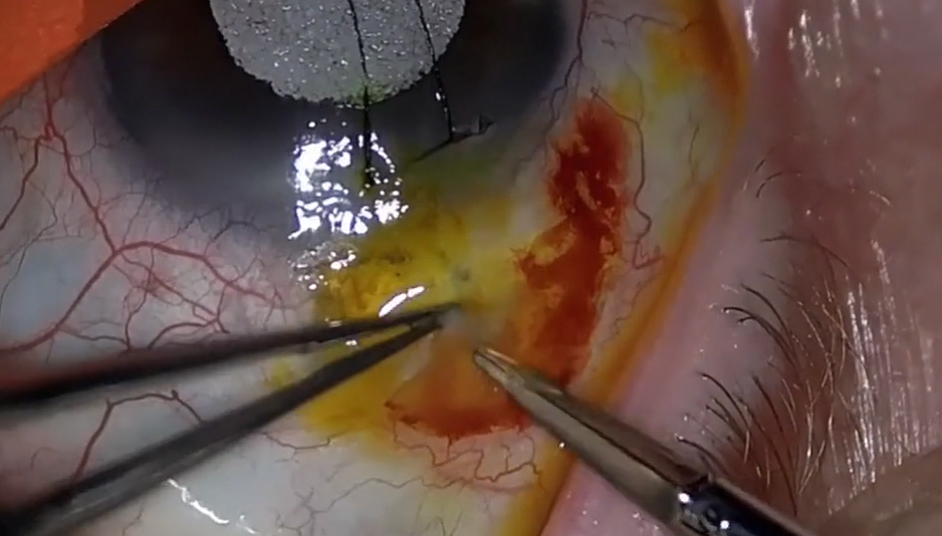
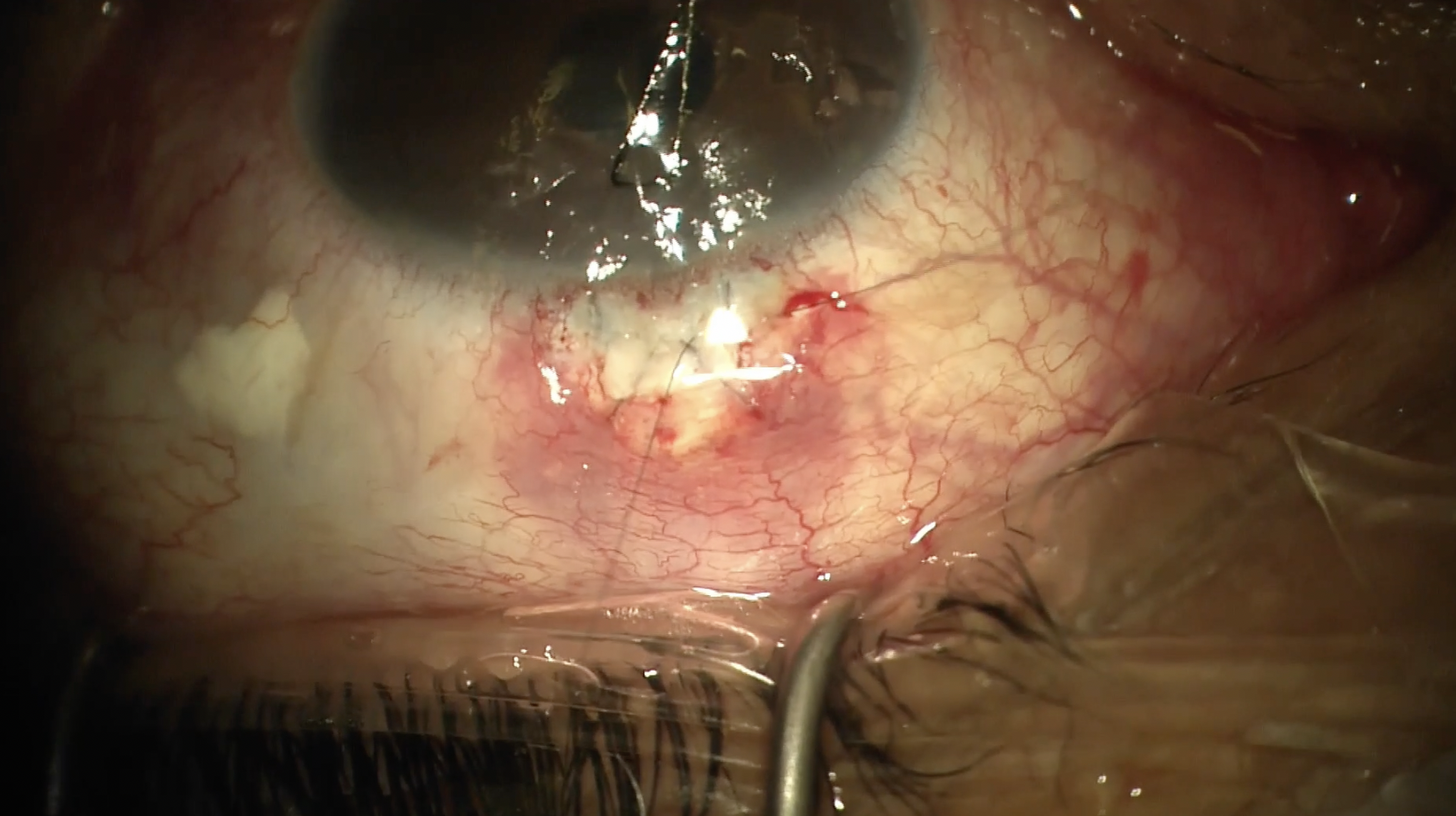
At this point, 24 mL of viscoelastic have been dispensed, so additional canaloplasty is performed by scrolling the wheel backwards, pushing down on the button each time. By the time the catheter was fully retracted, the button was pushed about 6 more times, so 18 more microliters of viscoelastic were dispensed. The catheter is re-scrolled all the way forward until the tip reaches the trab site and the microscope is zoomed out so the entire field can be seen and the handpiece cannula and catheter are pulled straight out of the para to perform an incisional goniotomy on the inferior 180° of the trabecular meshwork.
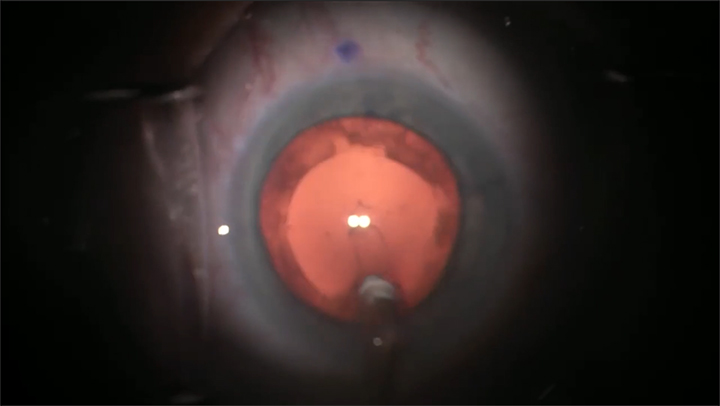
A second paracentesis was made so a 19-gauge bimanual I/A could be used to remove the Healon5. This can also be done with a coaxial I/A if the temporal wound is enlarged. The aspiration handpiece is removed and regular Healon is injected into the AC as the irrigation handpiece is removed. This maneuver is performed out of an abundance of caution to keep the AC maintained and prevent reflux bleeding while the paras are secured, after which point BSS on a cannula can be used to gently rinse the Healon out of the AC. At the end of the case the eye is left well pressurized to prevent reflux bleeding and intracameral antibiotic and subconscious decks are administered to prevent infection and reduce postoperative inflammation.
Thank you so much for watching my video. Please e-mail me if you have any questions and check out my YouTube channel for more surgical videos. GP
Other Videos From Series