For Glaucoma Physician's Surgical Pearls video series, Huda Sheheitli, MD, presents a technique for surgical revision of an exposed Baerveldt tube shunt associated with scleral melt. Transcript of the narration follows below:
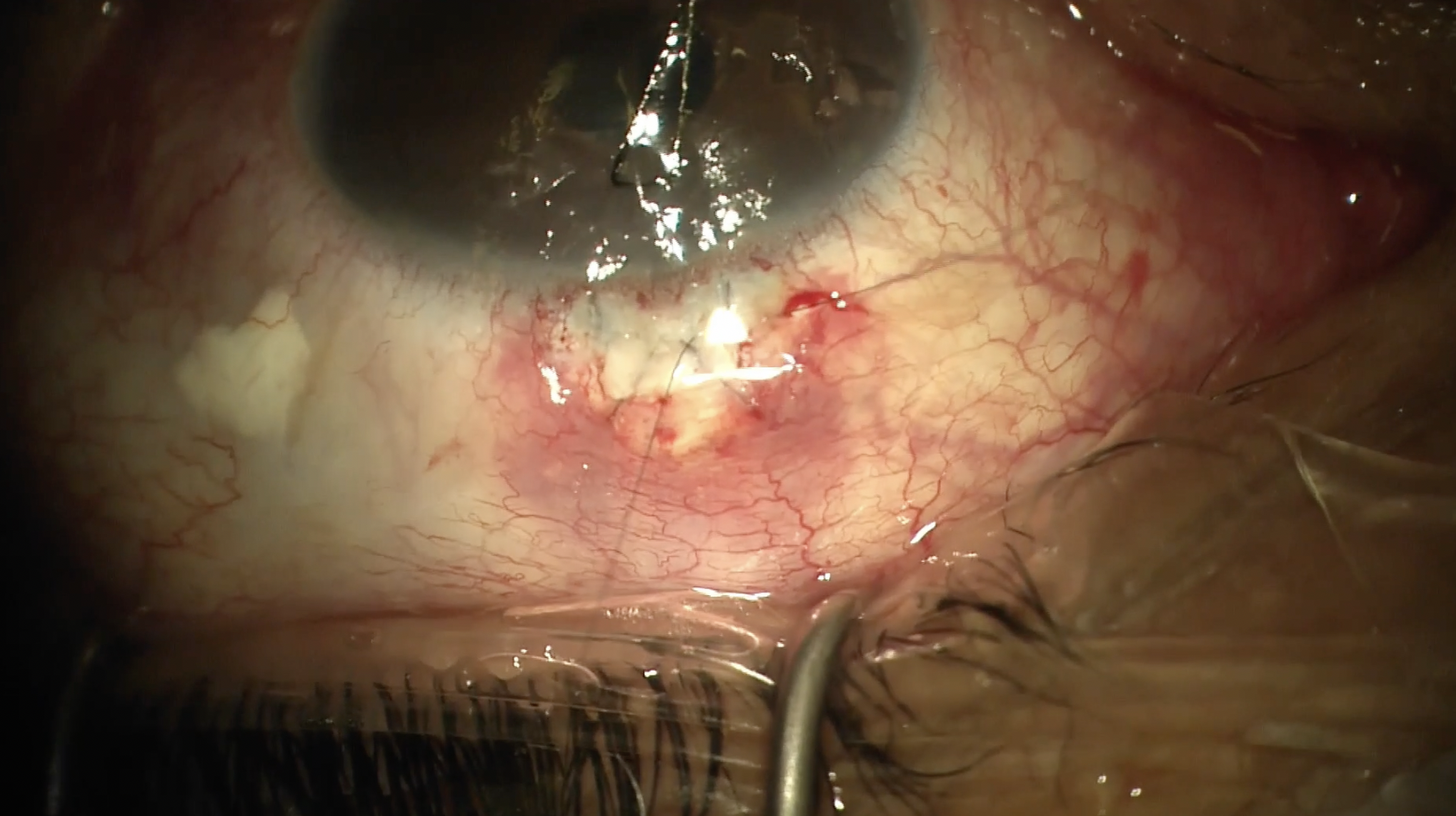
This is Huda Sheheitli, MD, a glaucoma specialist from University of Minnesota. This video presents the surgical revision of an exposed Baerveldt tube shunt associated with scleral melt. The patient is an 81-year-old male with severe primary open-angle glaucoma (POAG) in the right eye. Four years prior to presentation, he underwent Xen gel stent (Allergan/AbbVie) implantation with mitomycin C (MMC). Eight months postoperatively, he required bleb needling with additional MMC, followed by a second needling procedure 1 month later. Despite these interventions, intraocular pressure (IOP) remained uncontrolled, prompting implantation of a nonvalved Baerveldt tube shunt (Johnson and Johnson Vision) in the superotemporal quadrant. Postoperatively, the patient developed hypotony and presumed endophthalmitis, which was managed by the referring ophthalmologist with tap and inject, pars plana vitrectomy, and removal of the Xen gel stent. Three years later, he was referred to my clinic with tube shunt exposure and surrounding scleral melt.
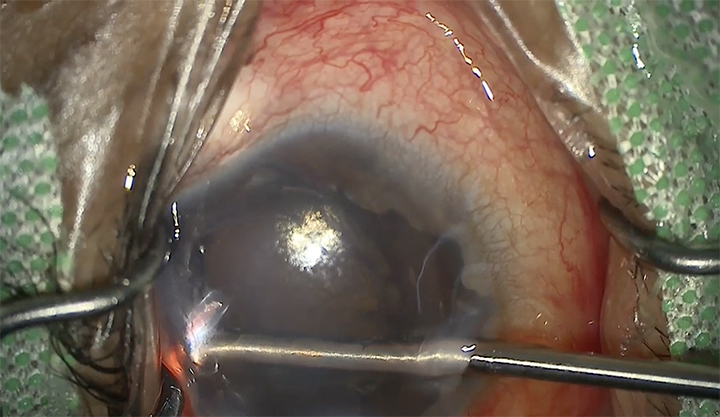
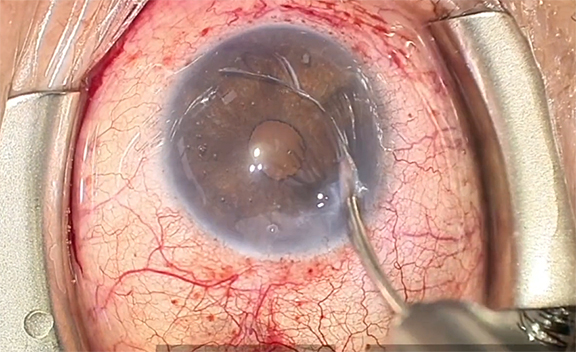
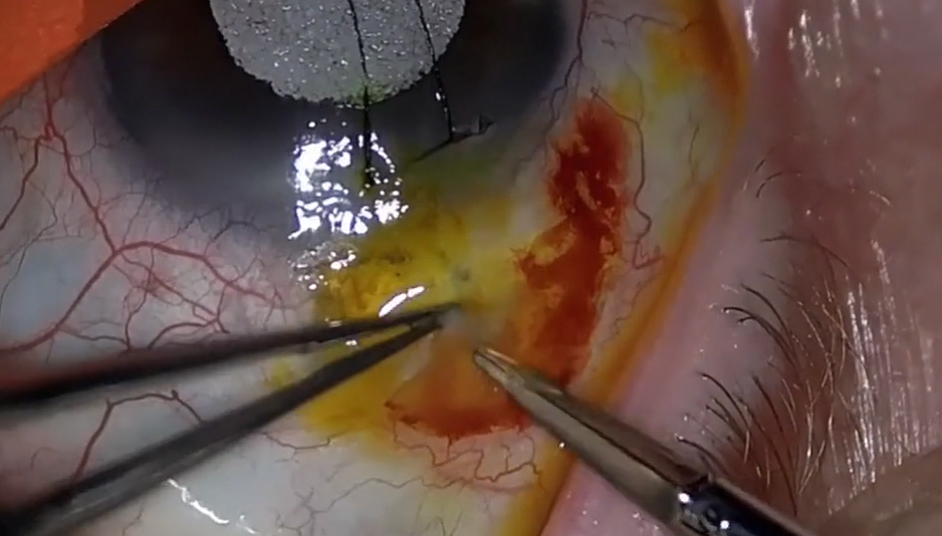
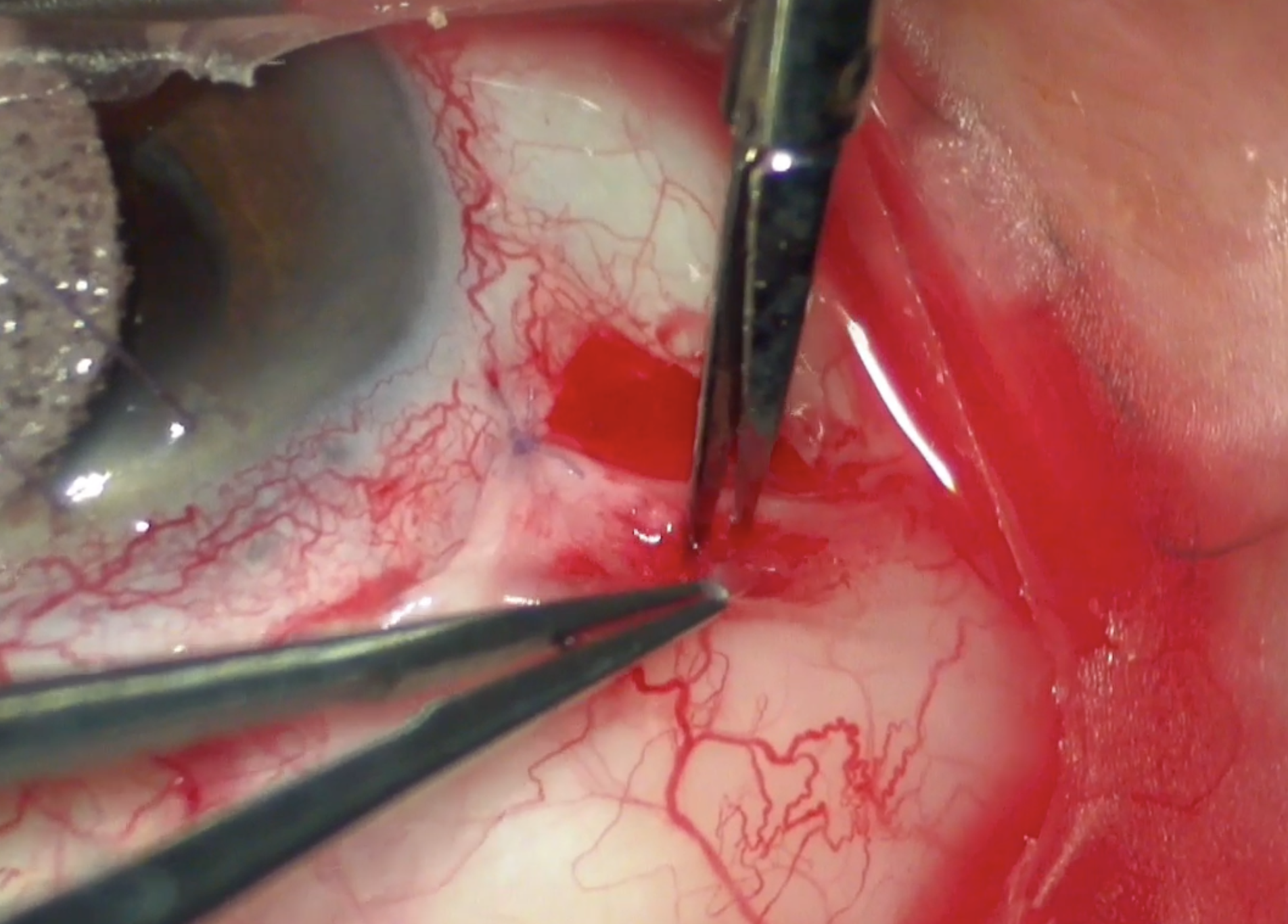
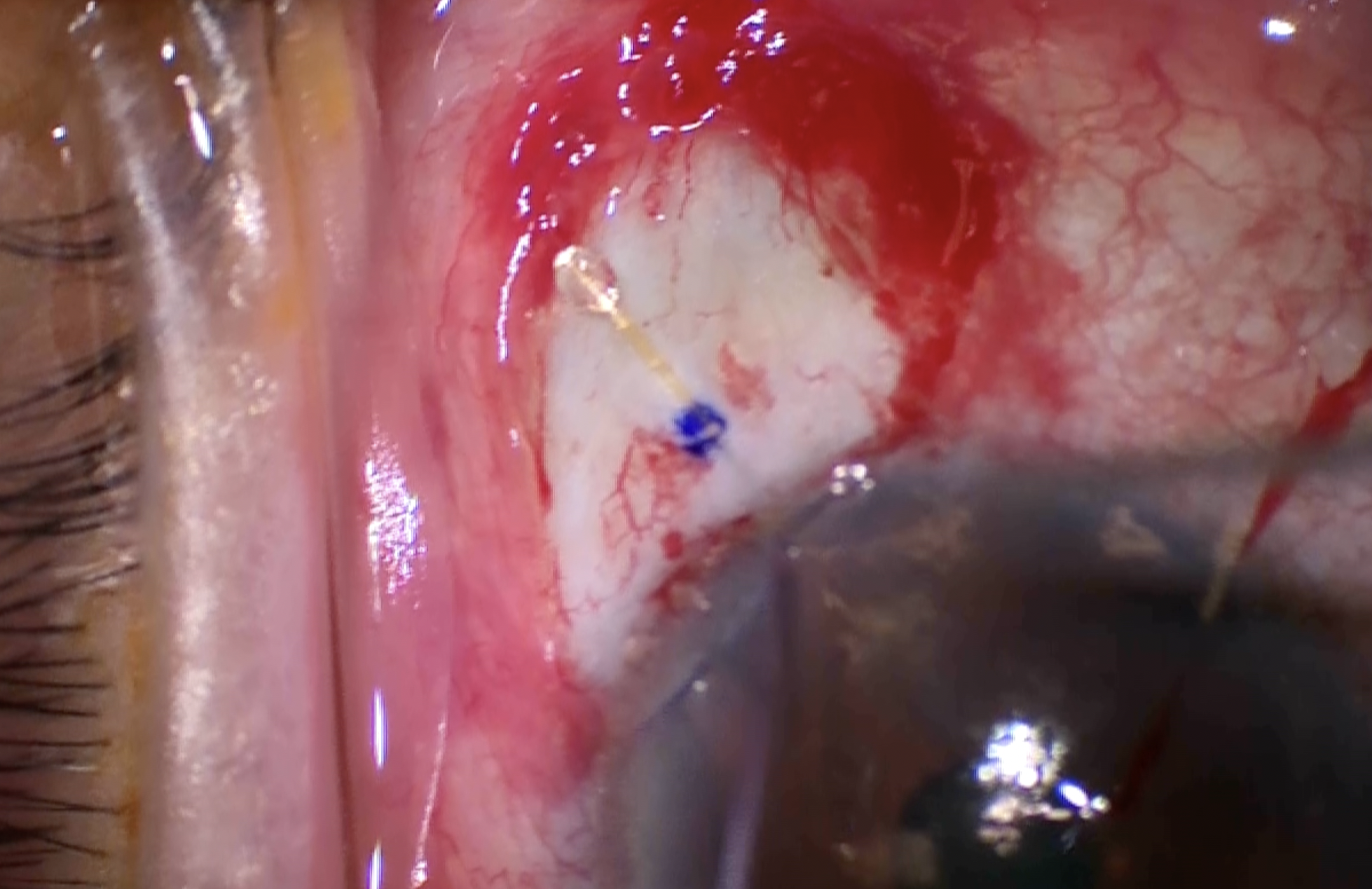
When planning surgical revision, it is important to assess the extent of conjunctival ischemia and the areas of scleral melt. In this case, there were 2 distinct areas of scleral melt and a broad region of ischemia devoid of healthy conjunctiva and vascular supply. Given the severity of the ischemia, I elected to remove both the tube and the plate, rather than attempt a revision using patch grafts.
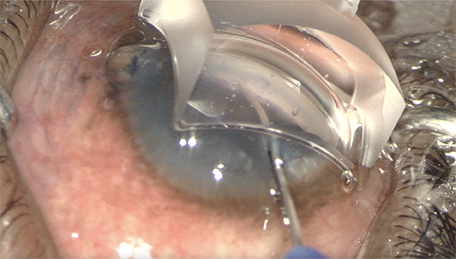
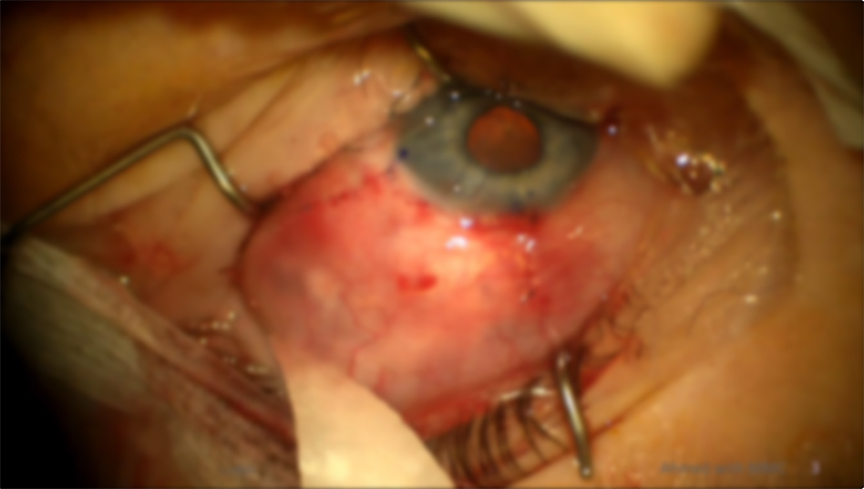
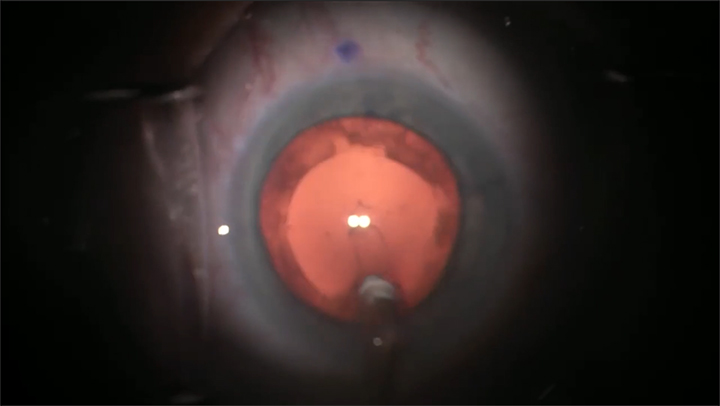
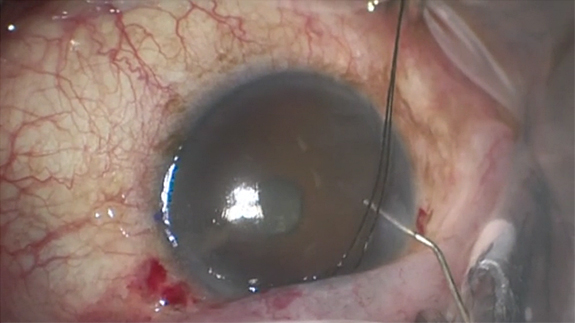
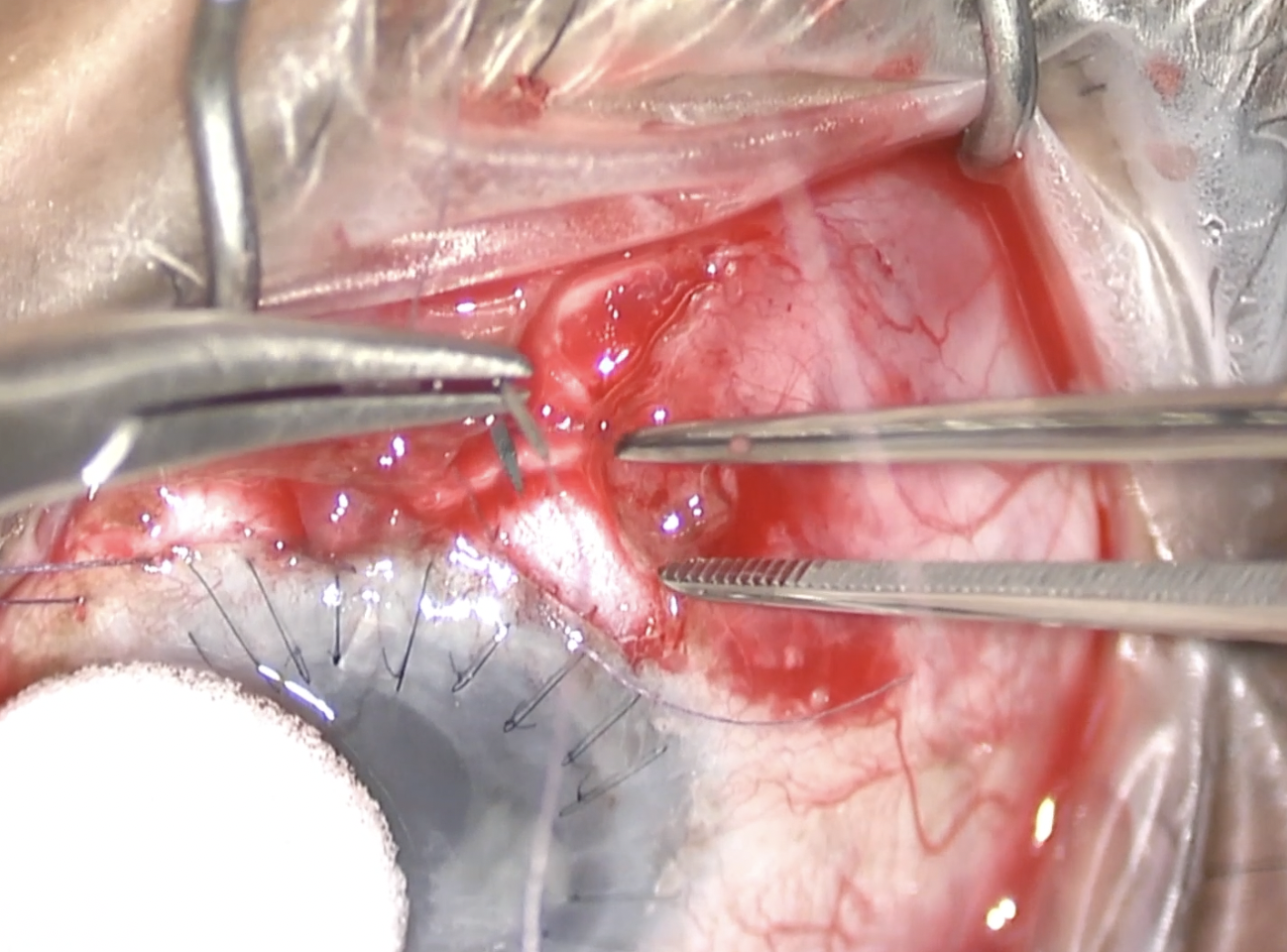
After placing a 7-0 Vicryl traction suture, conjunctival peritomy was performed. Paracentesis was created and the anterior chamber was formed with Healon. The tube was carefully freed from surrounding adhesions and removed from the anterior chamber. A small piece of scleral patch graft was then used to seal the sclerotomy, reducing the risk of leakage in the context of thin, ischemic sclera. Two additional scleral patch grafts were placed over the areas of scleral melt for reinforcement. The Baerveldt implant was removed after gentle dissection of the thick adhesions between the plate and the underlying sclera. Conjunctival blunt dissection was then carried out to ensure adequate mobilization and full coverage of the ischemic sclera. The peritomy was closed with 8-0 Vicryl sutures on a B-V needle.
Glaucoma surgery has evolved significantly, offering a spectrum of treatment options tailored to disease severity. Minimally invasive glaucoma surgeries (MIGS), including minimally invasive bleb-forming procedures like the Xen gel stent, provide safer, less invasive alternatives to traditional approaches. While outcomes are generally favorable, the long-term success of bleb procedures remains limited by subconjunctival scarring, making the use of antimetabolites like mitomycin C standard practice. MMC remains the most frequently used antifibrotic agent during glaucoma filtration surgery. Although MMC improves surgical success, it carries risks, and dosing strategies have shifted toward lower concentrations when feasible. Current evidence remains inconclusive on whether subconjunctival injection or sponge application yields better outcomes, though most surgeons use injections, typically ranging from 10 to 40 µg.1 To avoid side effects, perform MMC injection into the subtenon area at least 8 mm away from the limbus. At the time of surgical revision of MMC-induced ischemic conjunctiva and sclera, consider performing a large peritomy to allow for proper mobilization of the conjunctiva and achieve full coverage of the sclera. Additionally, consider using a small piece of the scleral patch graft to close sclerotomies to avoid postoperative hypotony and leak when dealing with an ischemic and thin sclera. Lastly, avoid placing glaucoma nonvalved tube shunt implants at the site of MMC-treated ischemic conjunctiva when possible. As more bleb-forming devices and subtenon MMC techniques gain popularity, careful surgical planning is essential, especially for secondary interventions such as non-valved tube shunt implants. In cases of significant or 360° ischemia, alternative strategies like cyclophotocoagulation or angle-based procedures may offer safer alternative to filtration surgery.
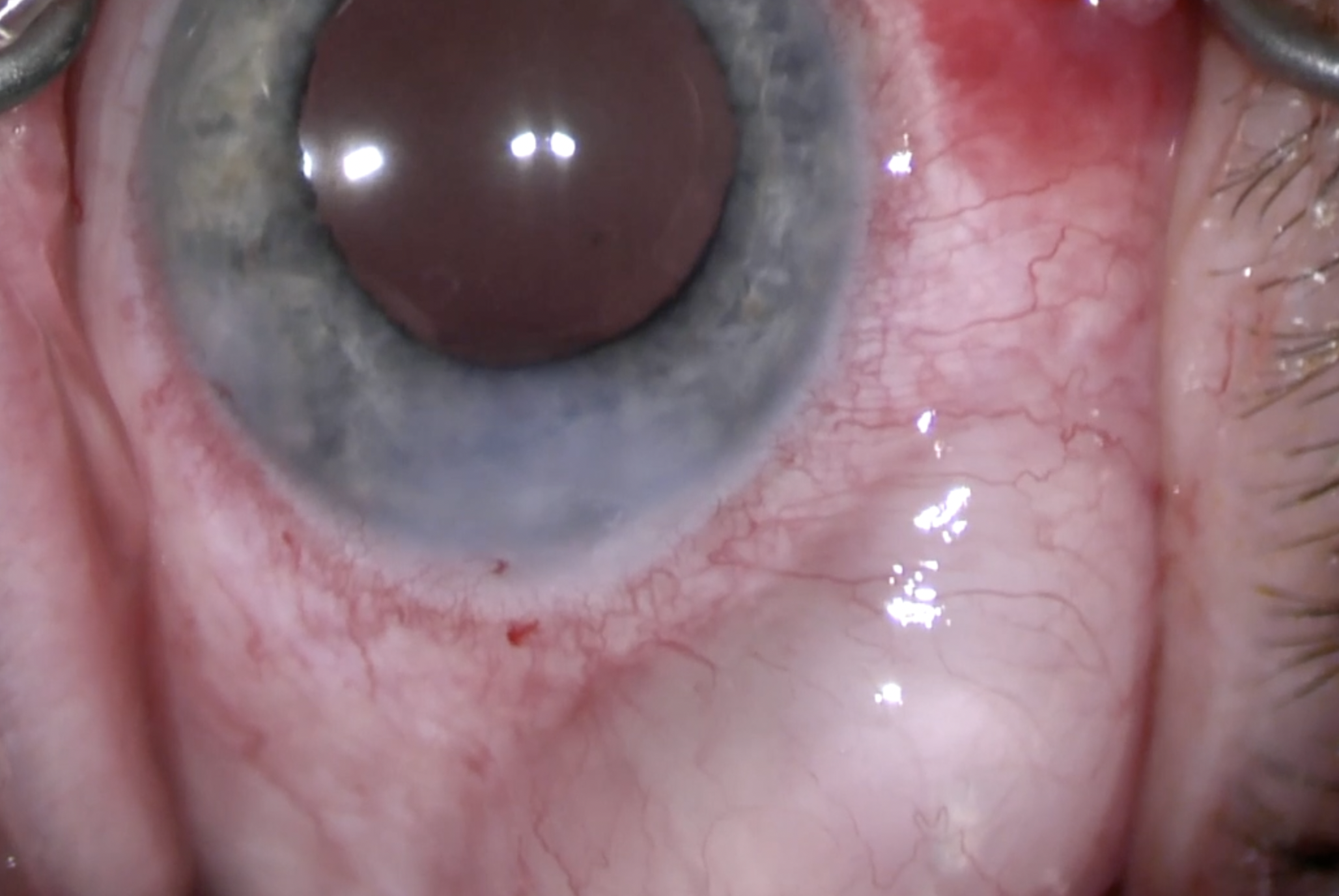
The patient continues to do well 1 year postoperatively, with fully covered sclera and controlled IOP in the mid-teens on 1 glaucoma eye drop medication, possibly due to ciliary body shutdown. GP
References
1. Sheybani A, Vera V, Grover DS, et al. Gel stent versus trabeculectomy: the randomized, multicenter, gold-standard pathway study (GPS) of effectiveness and safety at 12 months. Am J Ophthalmol. 2023;252:306-325. doi:10.1016/j.ajo.2023.03.026
Other Videos From Series