For Glaucoma Physician’s Surgical Pearls video series, Drs. Mehak Kalra, Samantha Goldburg, and Mary Qiu demonstrate proper placement of scleral spacers in a cyclodialysis cleft following canaloplasty and partial goniotomy to enhance the conventional and uveoscleral outflow pathways. Transcript of the narration follows below:
This is a case of a Hydrus (Alcon) removal, iTrack Advance (Nova Eye Medical) to enhance the conventional outflow pathway, and Allo-Flo scleral spacers (Allo-Flo Uveo; Iantrek) to enhance the uveoscleral pathway.
The patient is an 82-year-old man with primary open-angle glaucoma. He had previously undergone phaco-Hydrus in both eyes and then sustained an orbital floor fracture in the left eye after trauma. He presented to our glaucoma division seeking another opinion about what to do. His vision was 20/20 in the right eye and 20/30 in the left eye, and his pressure was 22 mmHg and 18 mmHg on 5 meds in both eyes. On gonioscopy, the Hydrus was well positioned in the right eye, but was malpositioned in the left eye, with the distal end popping through the trabecular meshwork (TM) and poking out into the anterior chamber (AC). This Hydrus malposition is also demonstrated on (UBM), where the Hydrus is clearly not in Schlemm’s canal. Optical coherence tomography (OCT) demonstrates worse glaucoma damage on the left than the right, and this is confirmed by the visual field showing an inferior hemifield defect on the left.
With the target IOP likely in the low-to-mid teens, we decided to offer him a chance to surgically enhance the conventional and unconventional aqueous outflow pathway before moving on to subconjunctival procedures like a trab, tube, or Xen. Therefore, we counseled him that we would remove his malpositioned Hydrus, use the iTrack Advance to perform a canaloplasty and a small goniotomy (but not a full GATT, given his aspirin use), and use Allo-Flo to promote extra outflow through the uveoscleral pathway.
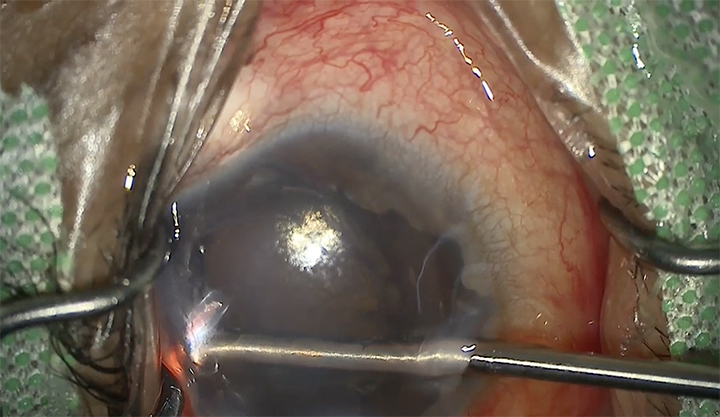
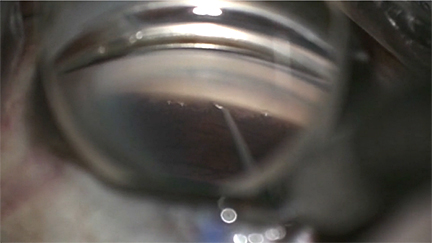
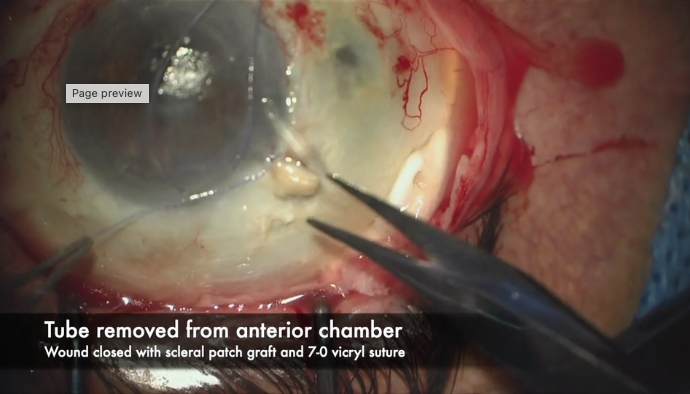
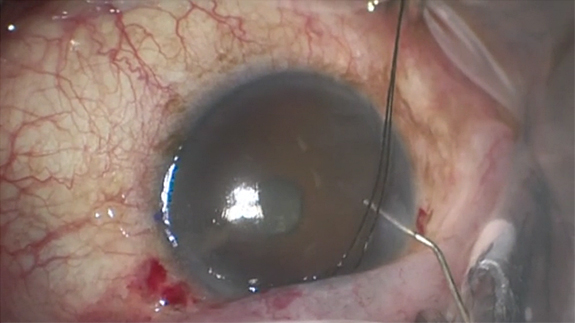
We’re sitting temporally and operating on a left eye. The paracentesis was made at 1:30, pointing at 9 o’clock for the iTrack Advance. Lidocaine and Myostat (Alcon) were injected into the AC, which was then filled with Healon5 (Johnson and Johnson Vision) to tamponade all bleeding. MST forceps were used to grasp the Hydrus, which fortunately was backed out easily. Once the Hydrus was mostly disengaged from the angle, it was released so the scope could be straightened. The Hydrus could be nudged into a better position with viscoelastic so it could be grasped head on with the MST forceps and pulled out of the paracentesis. The iTrack Advance was docked at this nasal otomy site. The catheter tip can be seen to be blinking and viscoelastic was dispensed to perform canaloplasty as it was advanced. There was an obstruction after approximately 3 clock hours, so we went the other direction. Viscoelastic was dispensed and another 4 clock hours of blanching can be seen before another obstruction was reached. The entire handpiece and catheter were pulled out of the eye, which performs a several clock-hour goniotomy.
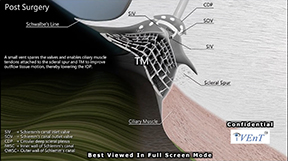
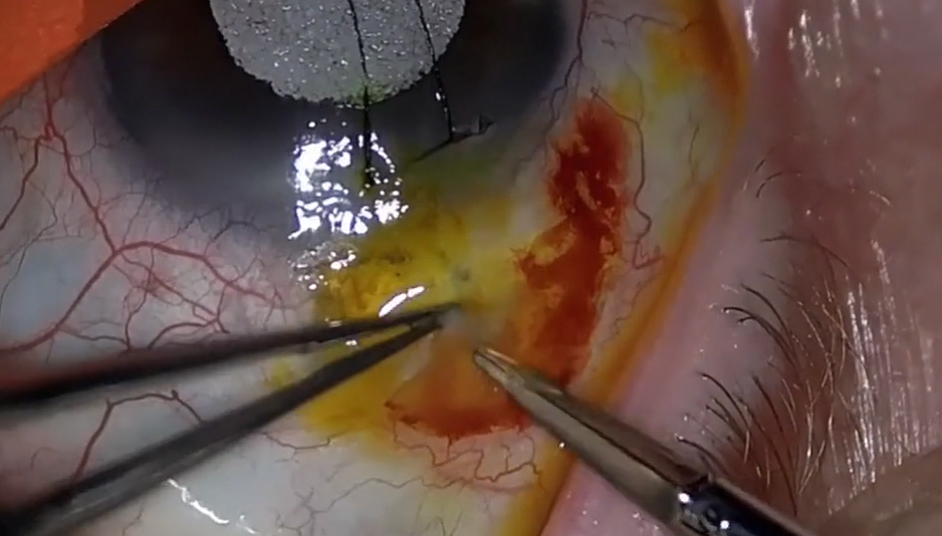
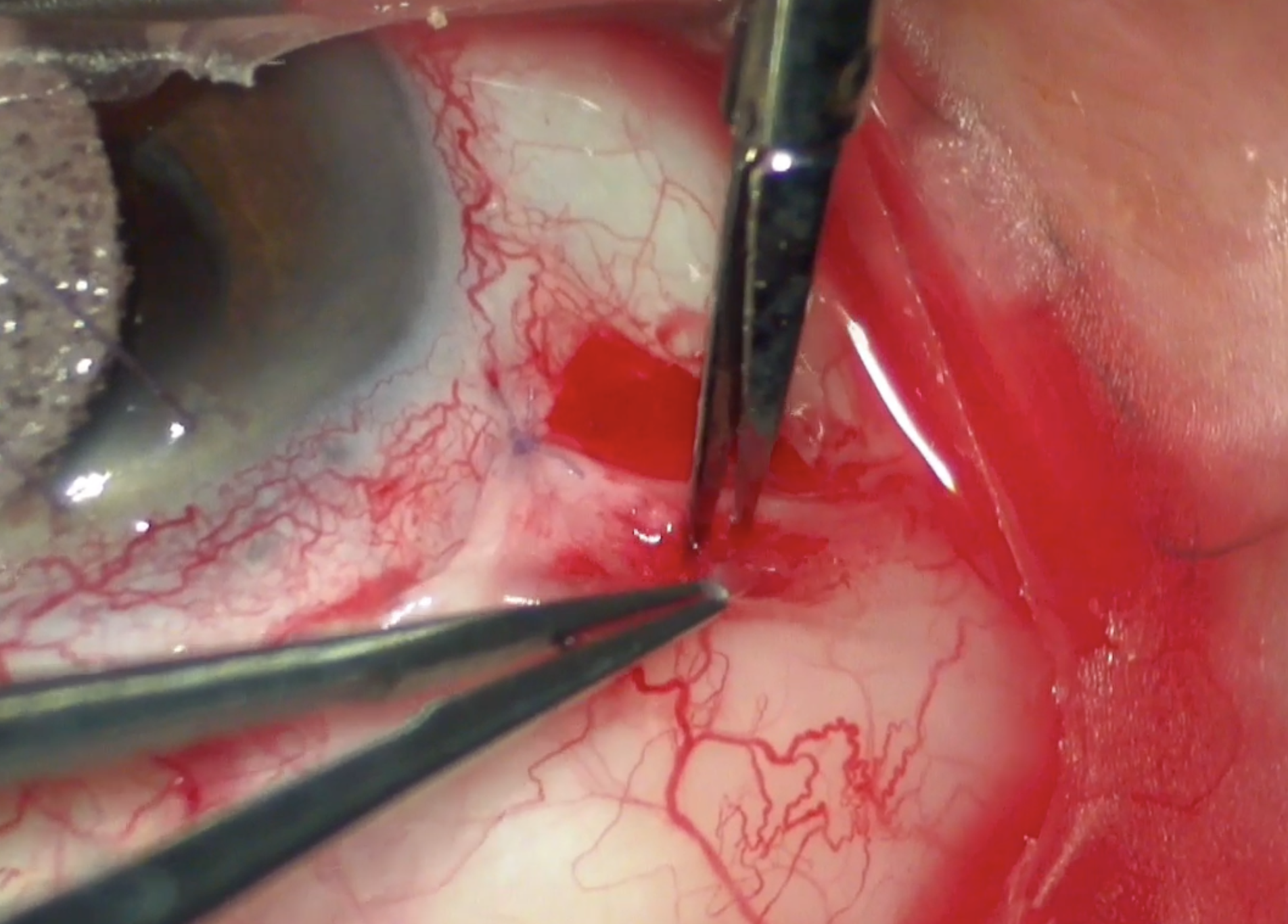
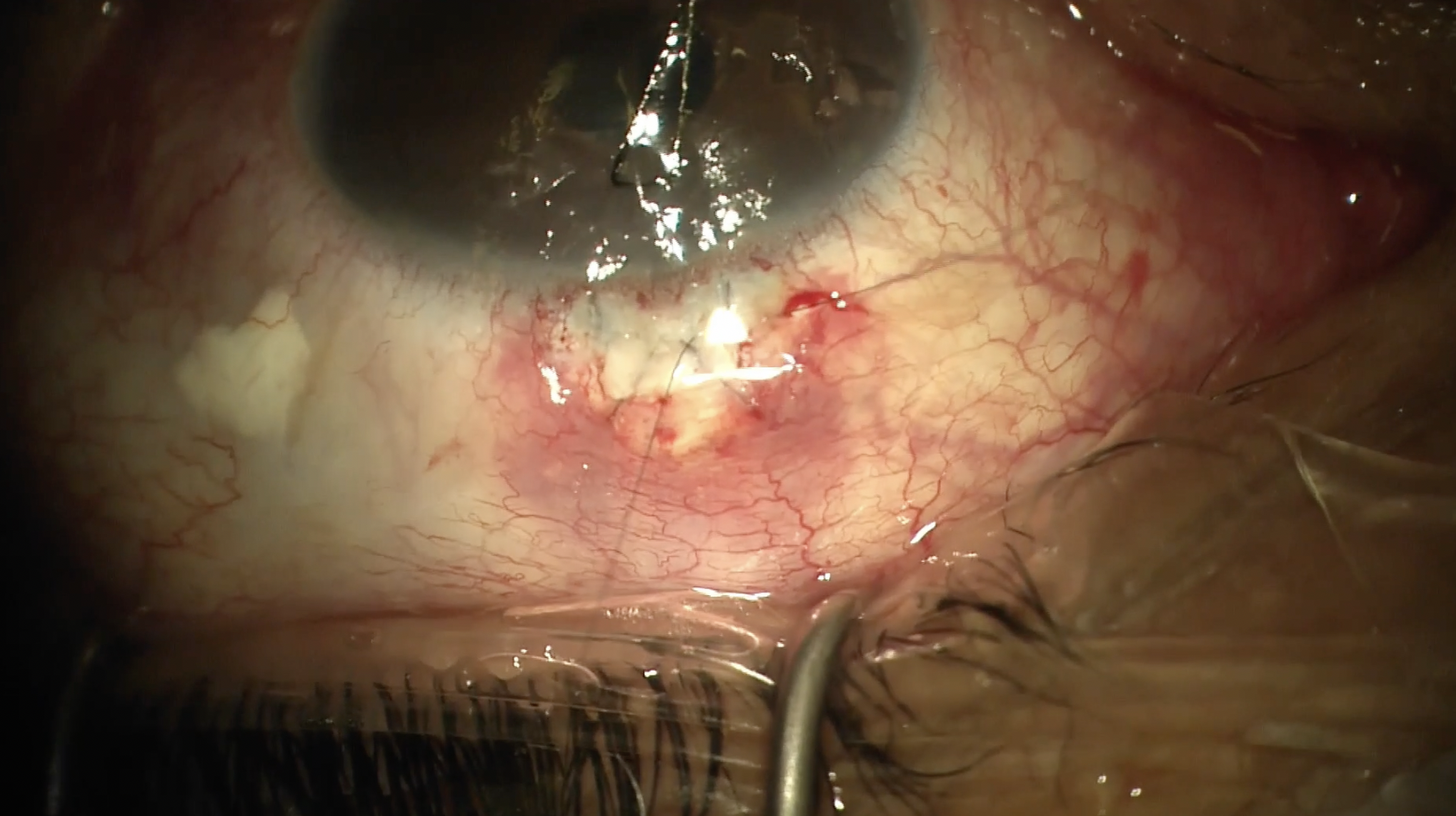
A 2.4 mm main wound was made for the Allo-Flo. A Provis cannula was used to create a cyclodialysis by gently peeling the circular and longitudinal fibers of the ciliary body off of the back wall of Schlemm. Viscoelastic can be directly injected into the cyclodialysis cleft while creating it to both widen it and to tamponade all bleeding. Despite this patient’s aspirin use, the very heavy Healon5 keeps the blood at bay and the view very clear.
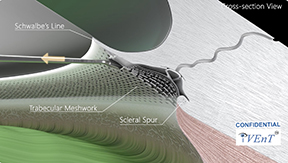
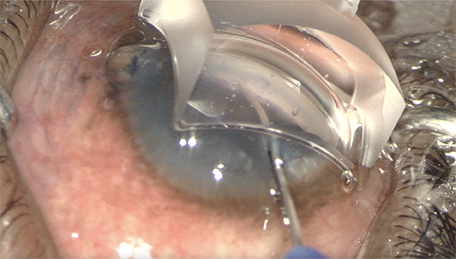
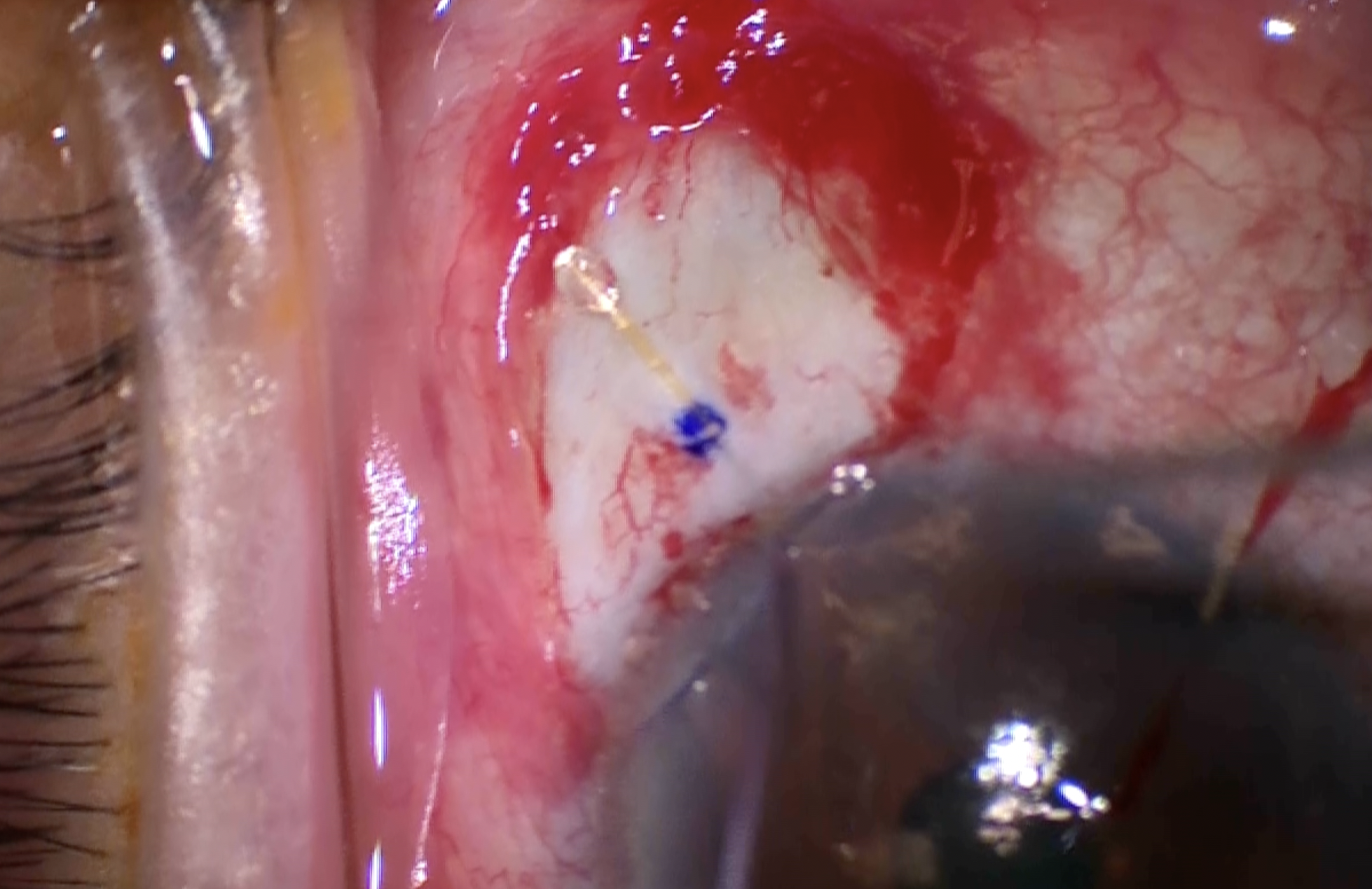
The Allo-Flo scleral spacer enters the eye and is docked into the cyclodialysis cleft that was previously created. It’s pushed forward until it’s engaged in the cyclodialysis cleft, taking care not to overimplant it. The white button on the inserter is pushed down and pulled back to retract the sheath and leave the Allo-Flo in place.
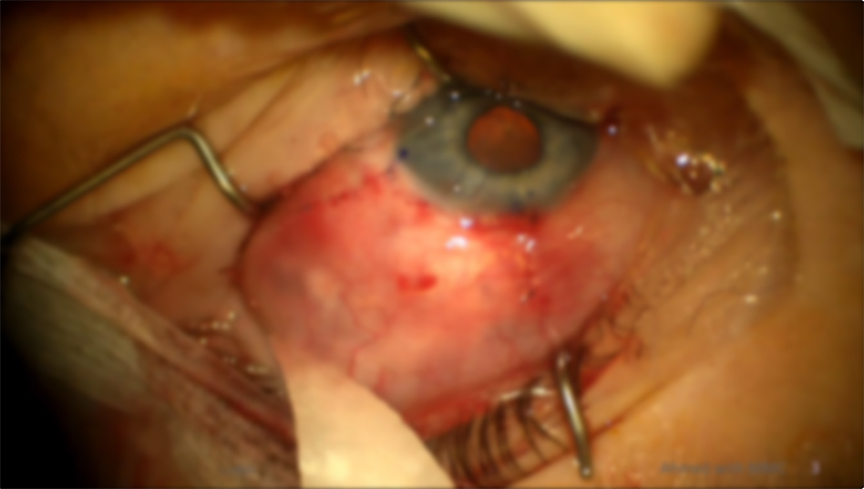
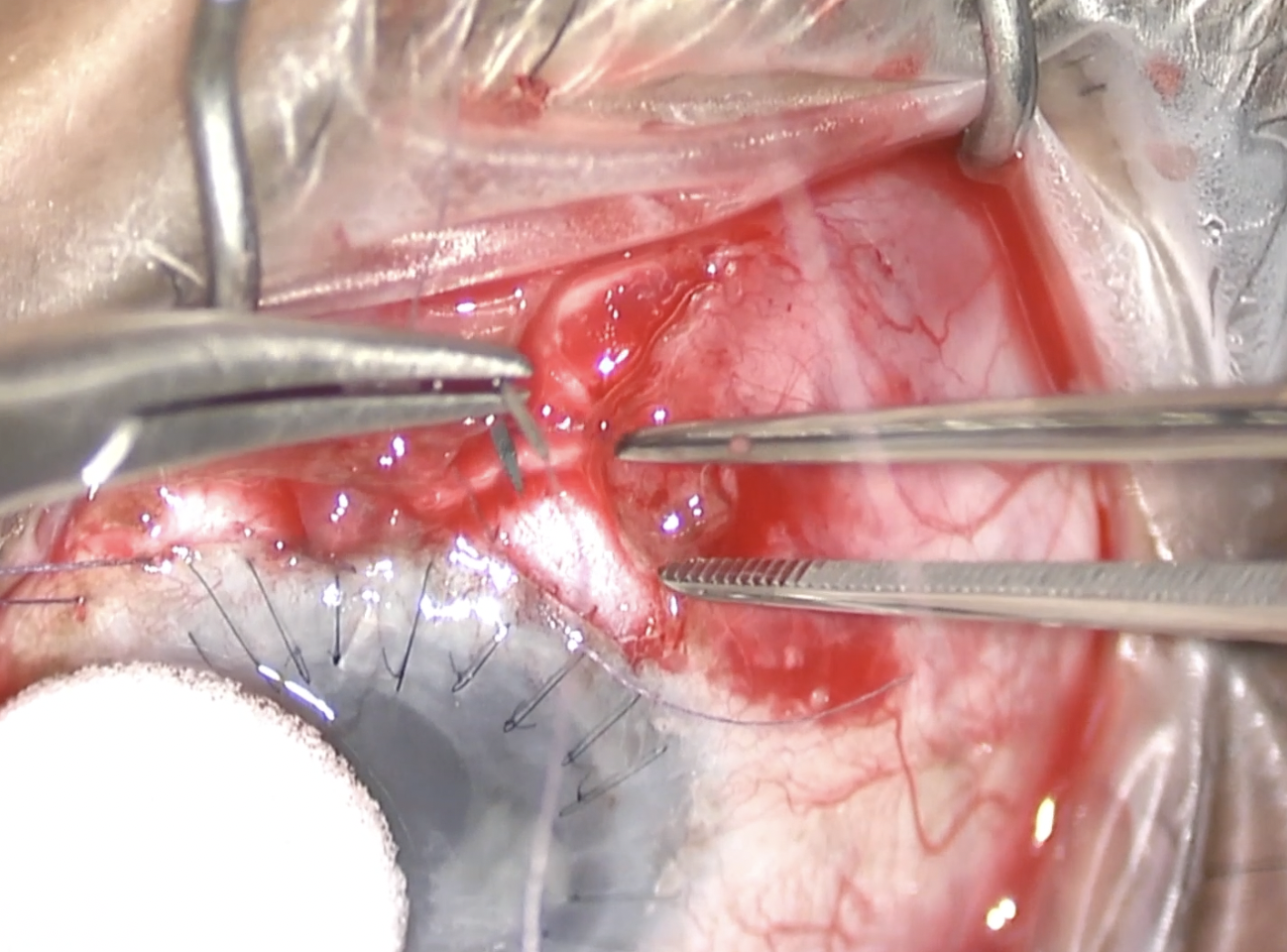
A second Allo-Flo scleral spacer is inserted in the same cyclodialysis cleft, approximately 1 spacer width away from the first Allo-Flo. Again, the white button on the inserter is pushed down and pulled back to retract the sheath from the spacer and leave the spacer in place. The second spacer was deployed a little too deep, so MST forceps were used to pull it back and nudge it slightly to the side. Healon was injected into the gap in between the 2 spacers to ensure there was adequate space between them. Both wounds were sutured out of an abundance of caution and some, but not all, of the viscoelastic was rinsed out of the AC. Some viscoelastic was purposely left in the AC to dampen the amplitude of IOP drop and reduce hypothetical reflux bleeding from the goniotomy site. The second Allo-Flo had retracted somewhat into the AC, so it was nudged deeper into the cyclodialysis cleft. The wounds were hydrated and confirmed to be watertight, and the case was complete.
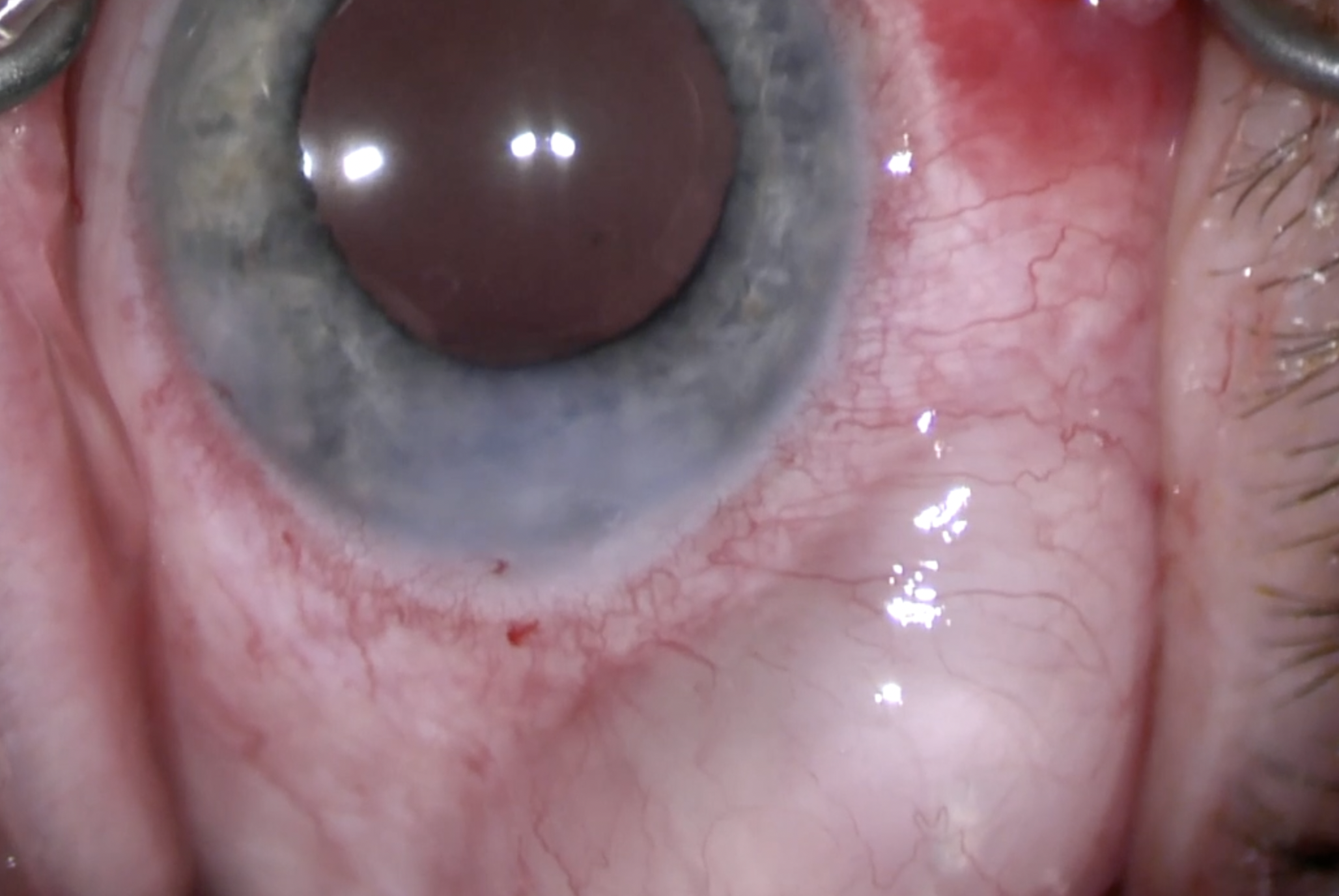
By postop week 4, the pressure was 11 mmHg on 4 meds. (The baseline had been 18 mmHg on 5 meds). The Allo-Flos were well positioned with a small gap in between the 2 spacers, and UBM confirms there was fluid in the cyclodialysis cleft.
Thank you so much for watching our video. Our Cleveland Clinic glaucoma fellow, Dr. Sam Goldburg, performs the removal of the Hydrus, the forehand iTrack Advance, the creation of the cyclodialysis cleft, and the insertion of the second Allo-Flo spacer. Our PGY2 resident, Dr. Mehak Kalra, performed the insertion of the first Allo-Flo spacer. We hope you’ll consider performing a combination of iTrack Advance and Allo-Flo for patients who could benefit from an enhancement of their physiologic conventional and unconventional outflow pathway. GP

Other Videos From Series