For Glaucoma Physician's Surgical Pearls video series, Ariana Levin, MD, and Albert Bargoud, MD, share a case of a same-quadrant Baerveldt 250 to Ahmed exchange. Transcript of the narration follows below:
This is Ariana Levin with Albert Bargoud at New York University.
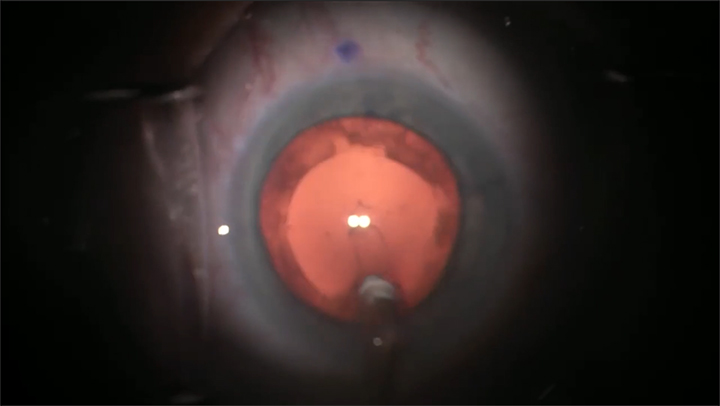
This is a patient with pseudoexfoliation glaucoma who underwent placement of a Baerveldt 250 shunt ligated with a 7-0 vicryl. When the tube opened at postop week 6, he developed hypotony with choroidal effusions, recalcitrant to multiple AC fills and local and oral steroids. At postop week 8, he underwent surgical revision.
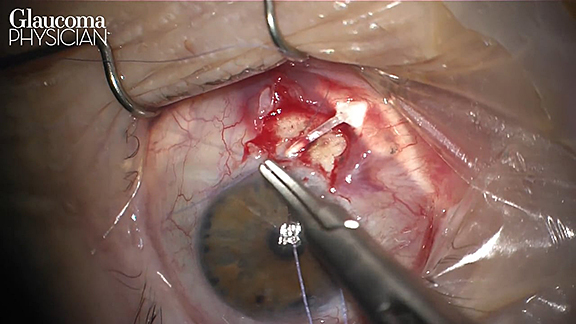
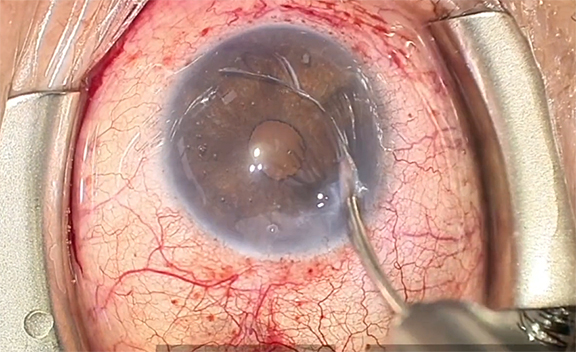
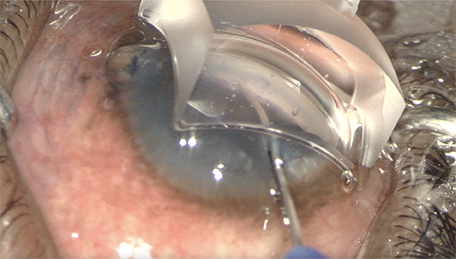
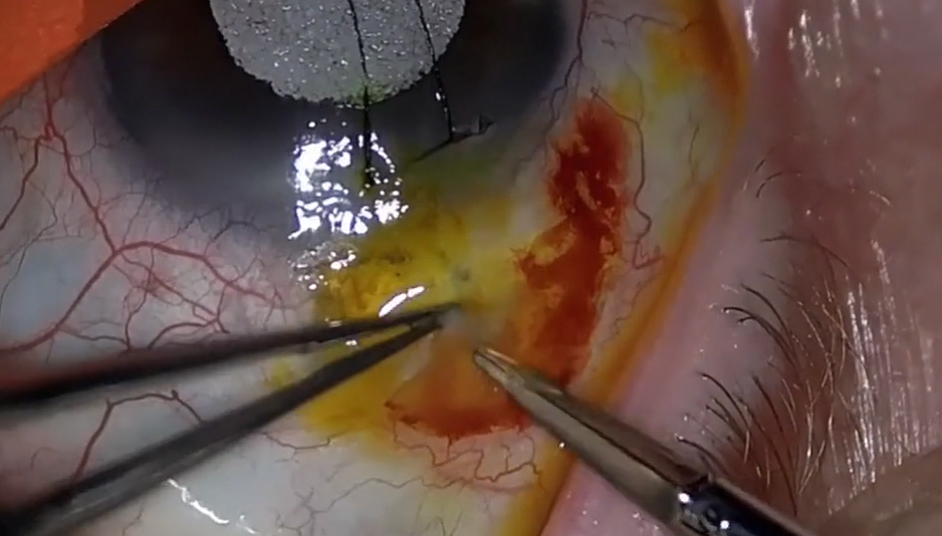
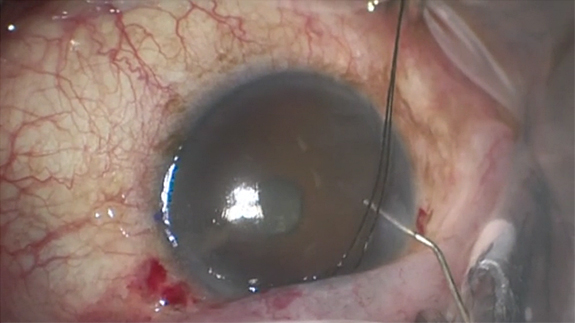
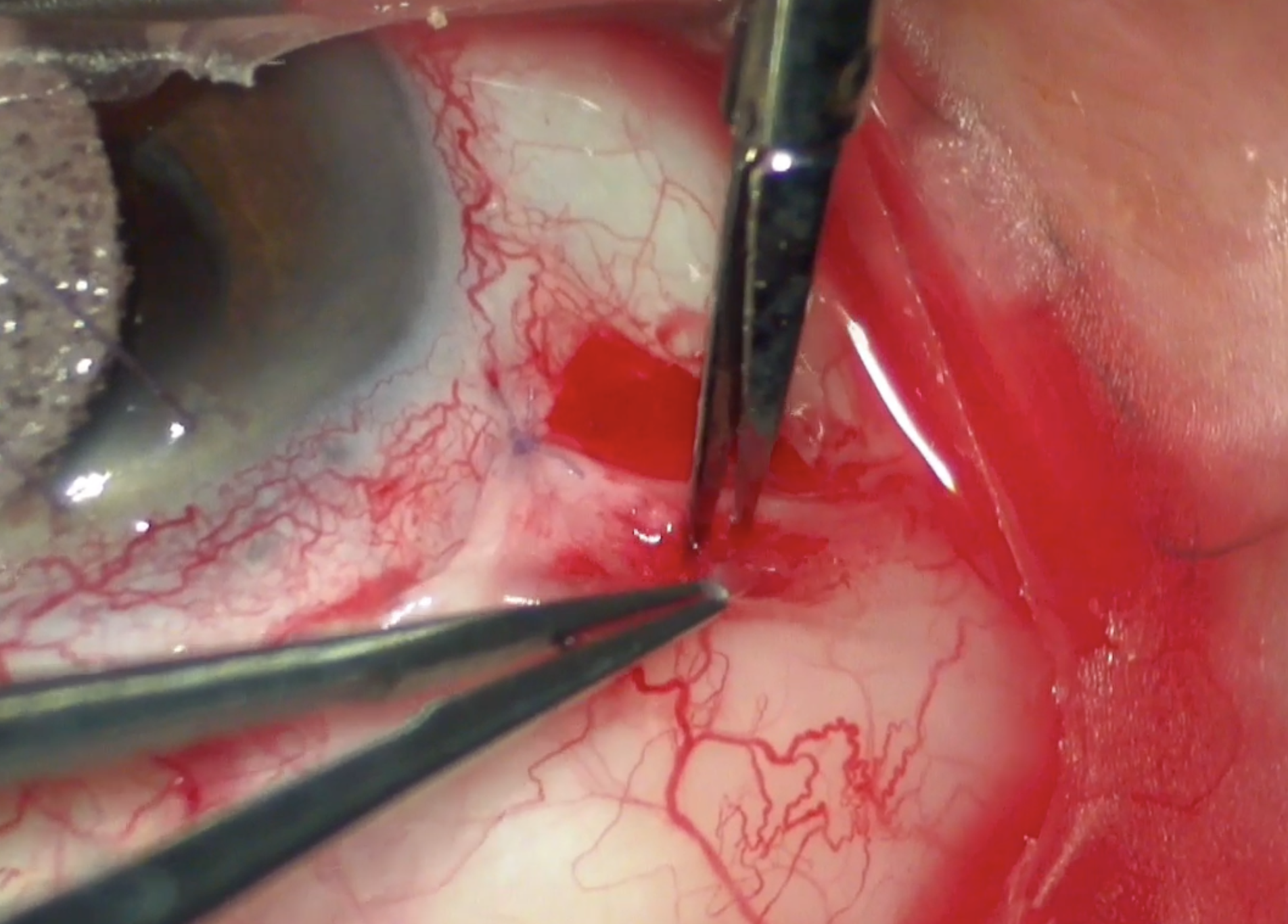
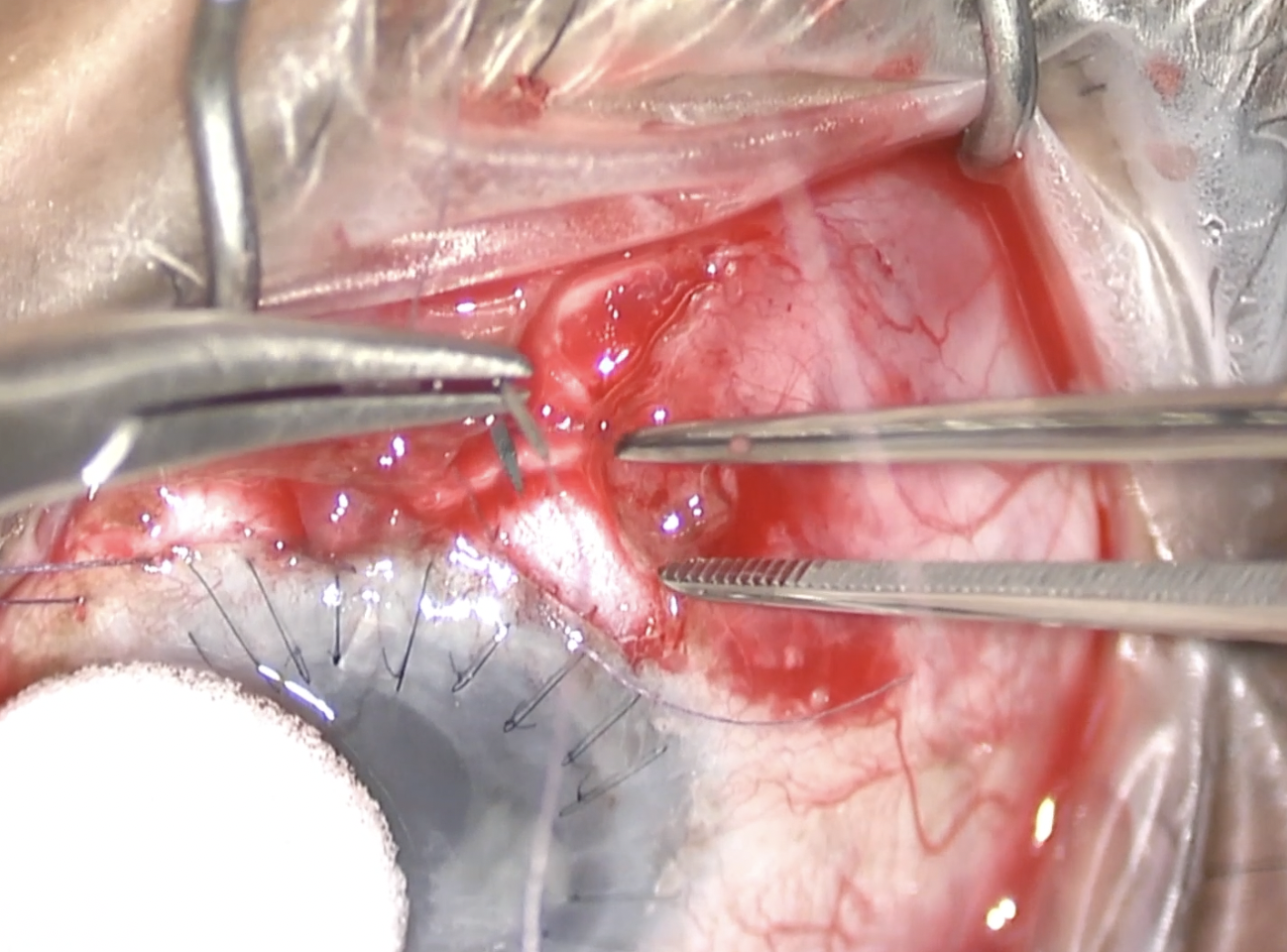
At the start of the case, the leading edge of the prior peritomy was noted to be free, indicating it had not healed previously. A paracentesis was made and the flat AC was stabilized with OVD. After placing a traction suture, blunt dissection was used to easily reopen the peritomy. Cautery was used for hemostasis. Relaxing incisions were made.
The surgical plan was to tie off the Baerveldt if a capsule had formed, or exchange it for a valved tube if a capsule had not formed. There was no capsule.
Fibrosis was noted only at the sites of prior vicryls — the ligation suture and some peritomy edges.
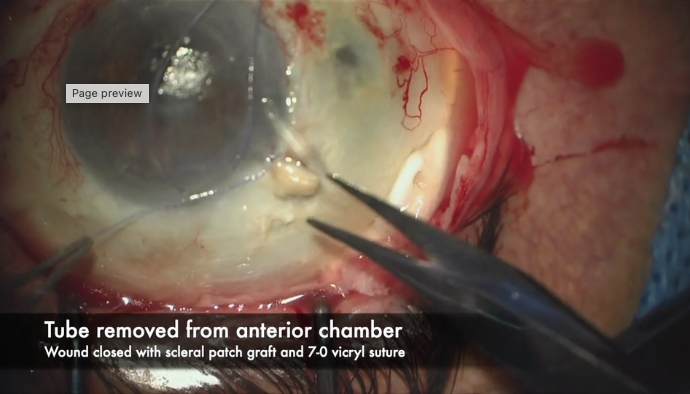
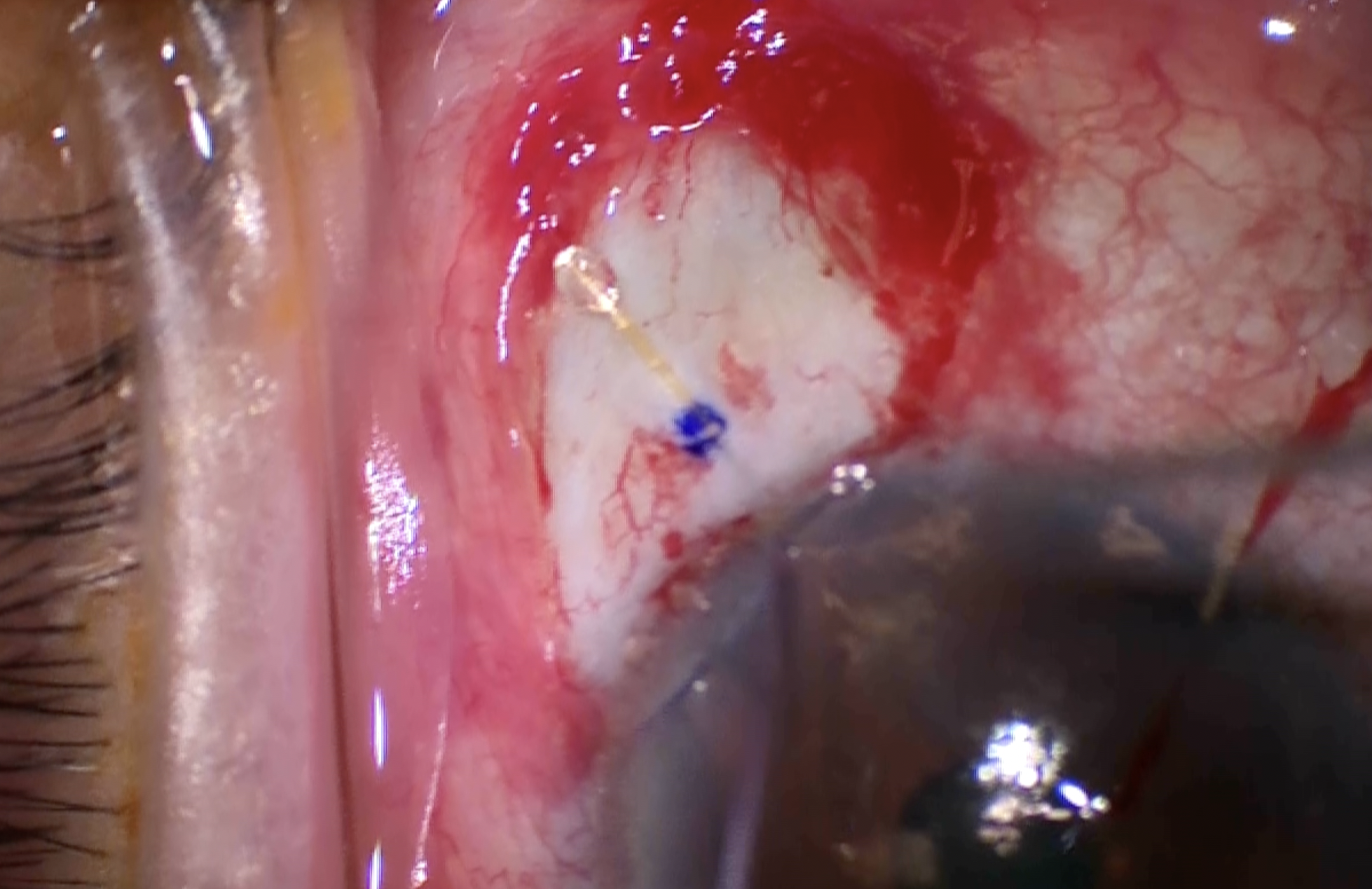
The Baerveldt was easily explanted; anchoring stalks had not formed through the plate holes.
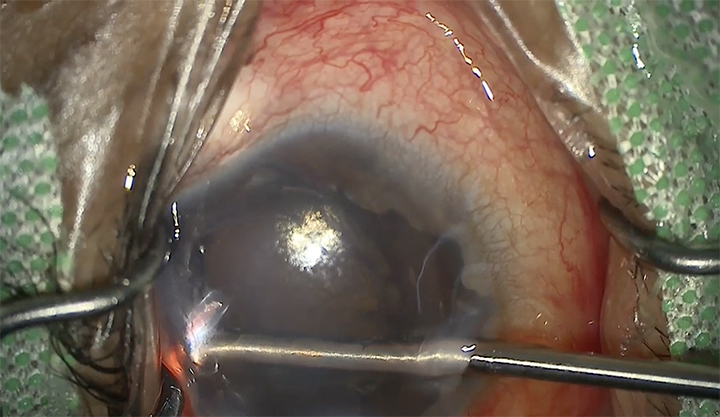
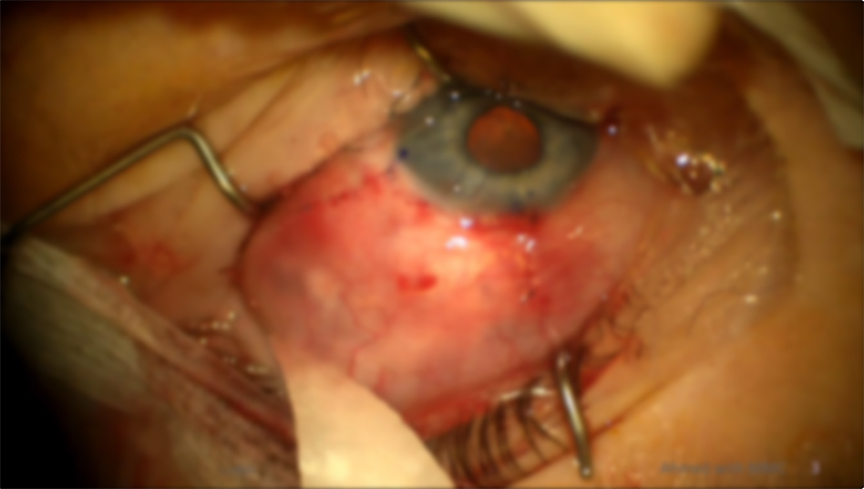
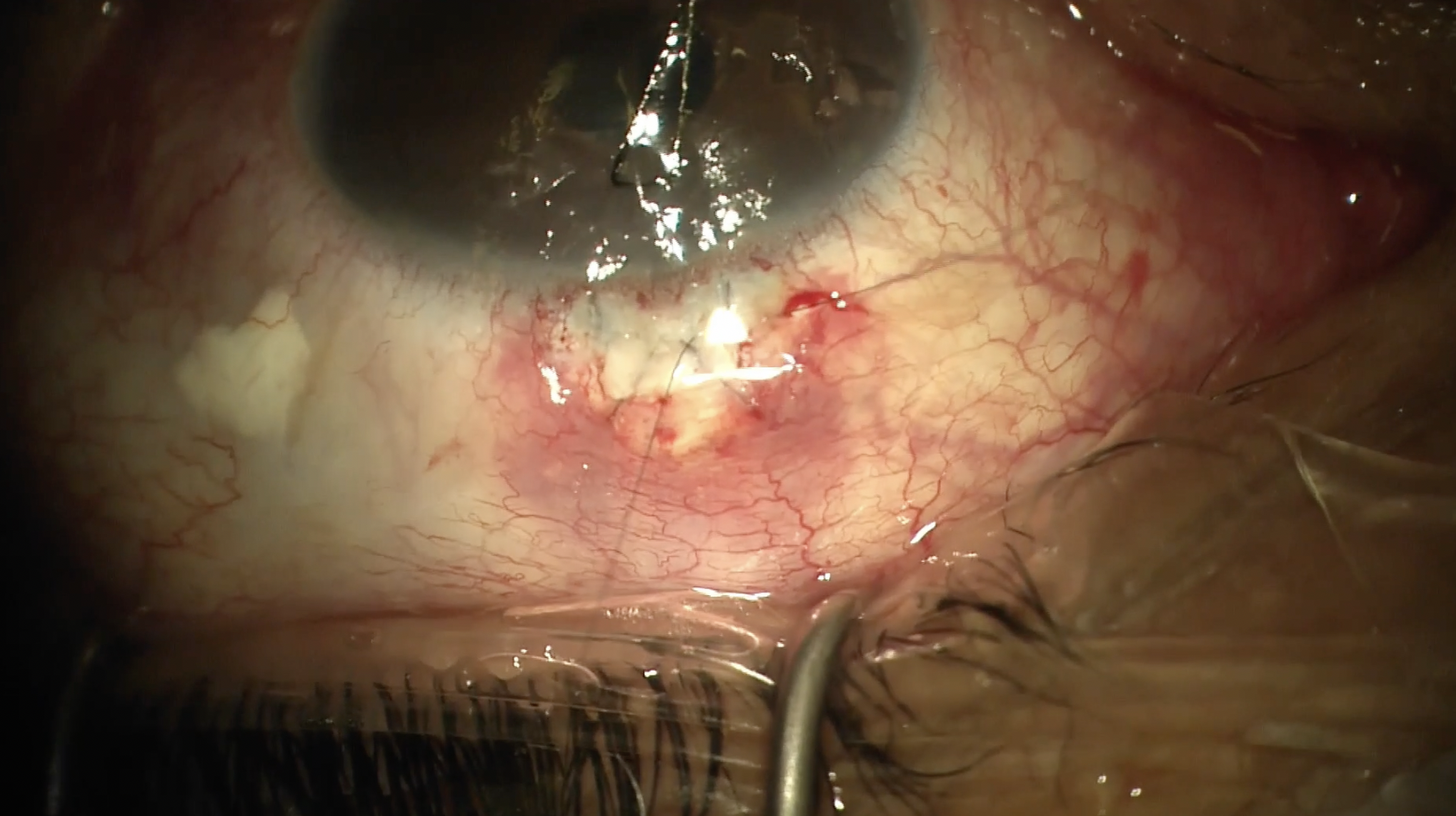
An Ahmed FP-7 was placed. The Baerveldt plate had been anchored with vicryl; now a nondissolvable Prolene was used instead to ensure long-term stability. The tube was ligated with 7-0 vicryl to allow for resolution of hypotony. The tube position was also secured with nylon. A corneal patch graft was placed, and then the peritomy was closed. A running vicryl with episcleral bites was used to close the relaxing incisions. Nylon in a running mattress suture was placed at the limbal edge.
Effusions were then drained.
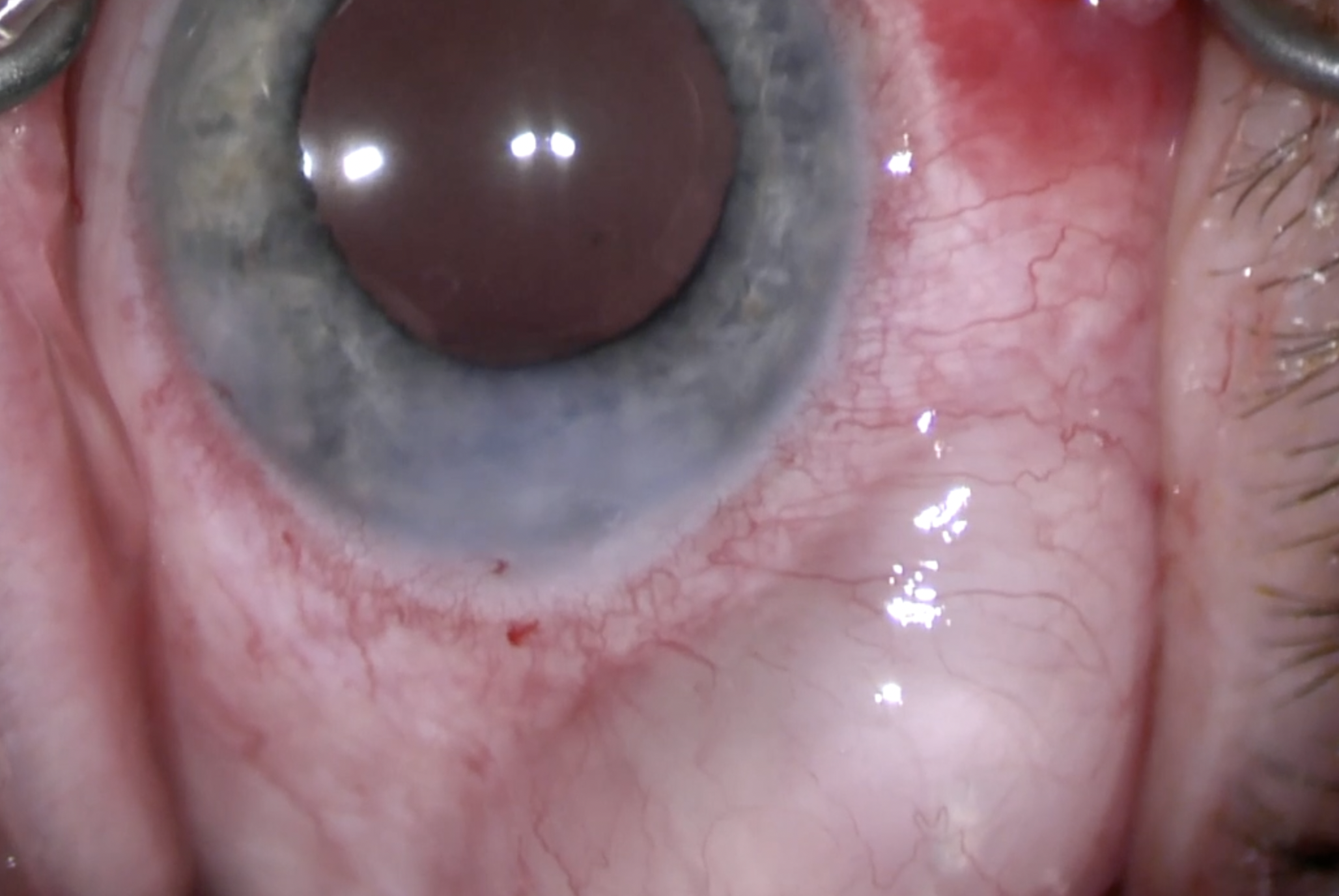
On postoperative day 1, IOP was 50 with a deep AC and no posterior effusions. After AC tap and addition of timolol, the eye stabilized.
Thank you for watching this video, highlighting how the patient’s propensity for healing, scarring, and fibrosis can guide decisions in revision surgery, the choice of implant, and the choice of sutures. Please email if you have questions. GP


Other Videos From Series