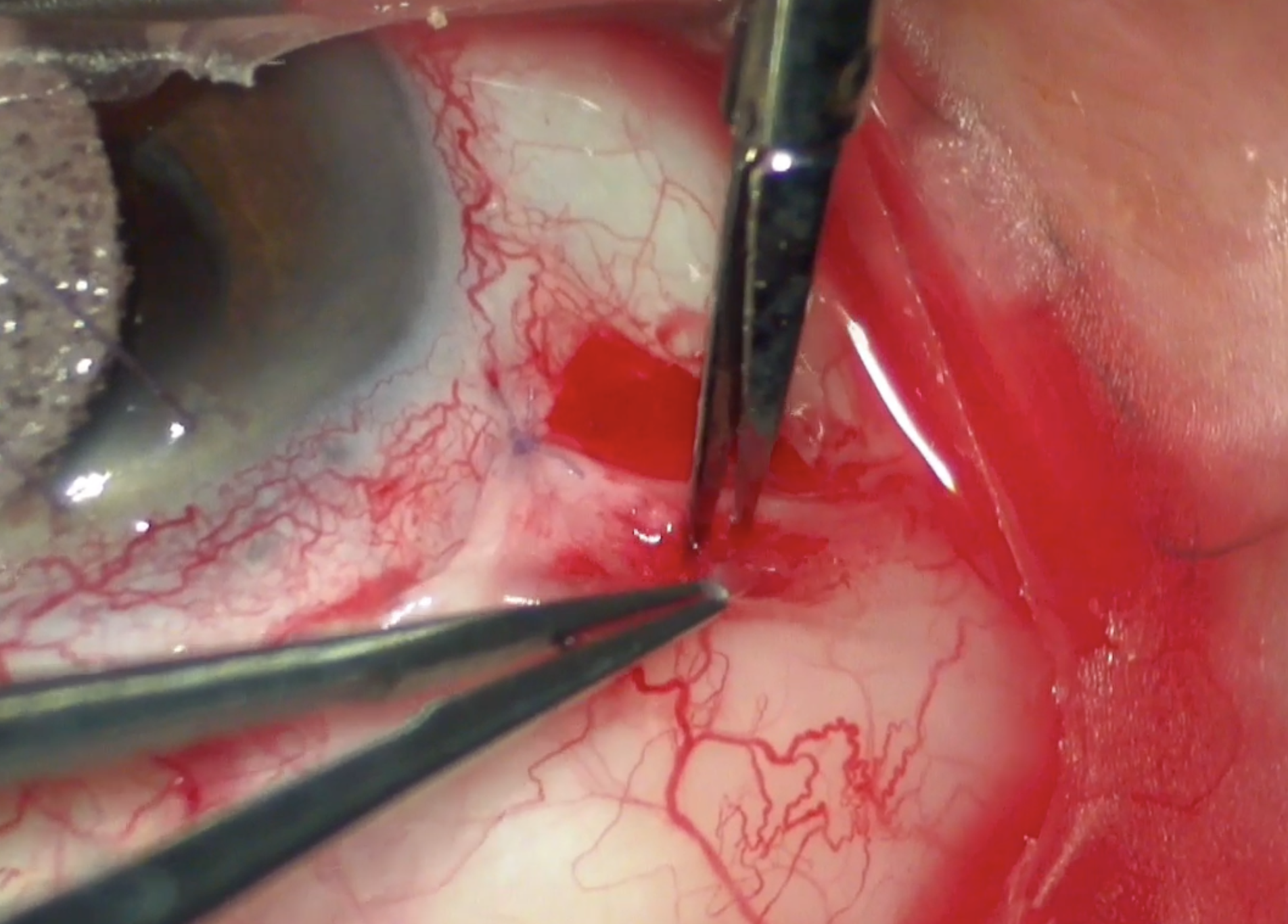
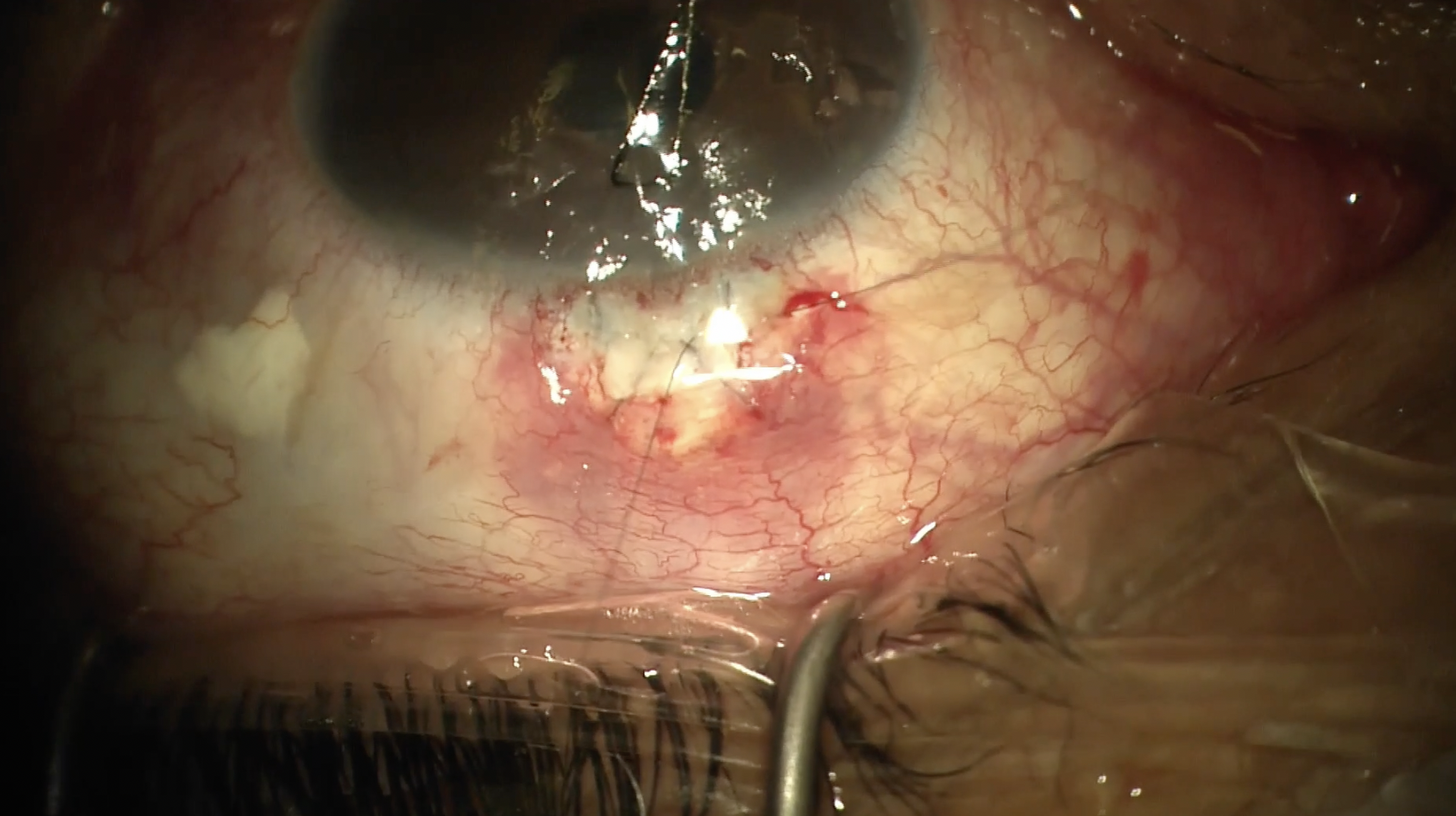
This video demonstrates my technique for an external Xen (AbbVie). Here, a radial incision is made supranasally, and the incision is carried out for about 3 clock hours. This allows us to get into the sub-Tenon space. Here, Tenons is being grabbed and then the sub-Tenon space is being dissected with blunt Westcott scissors.
Dissection is being carried out both posteriorly, nasally, and superiorly, so that there is plenty of space for a nice posterior bleb to form. You'll see later in this area we will apply large mitomycin sponges to allow for broad application of mitomycin to the sub-Tenon space.
These are allowed to sit for 2 minutes and another 0.2 mL of mitomycin is injected at about a minute to allow for additional mitomycin application. This mitomycin is 0.4 mg/cc concentration. For microshunts such as the Xen, the use of high-dose mitomycin is very important for bleb success.
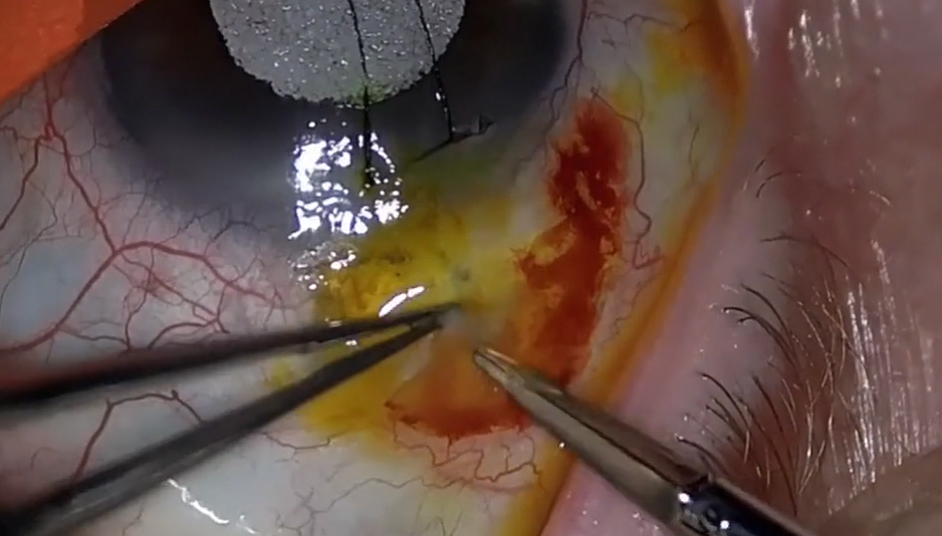
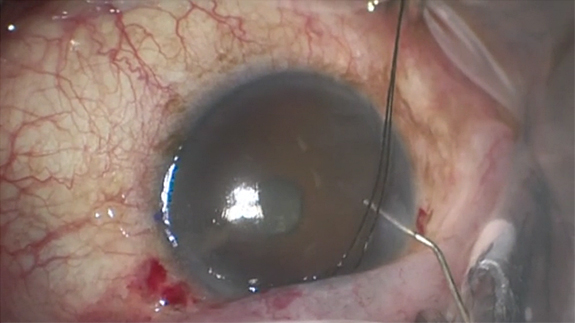
Here the sponges are being removed from that sub-Tenon space, and the area is being copiously irrigated with BSS solution. Cautery had already been applied here, and now we're using a bent 30-gauge needle that's been marked.
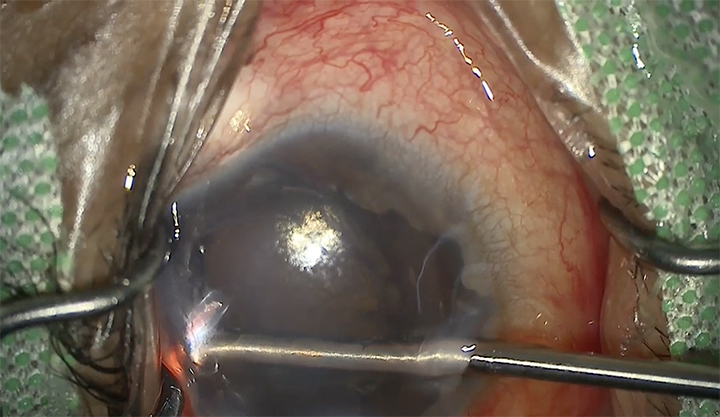
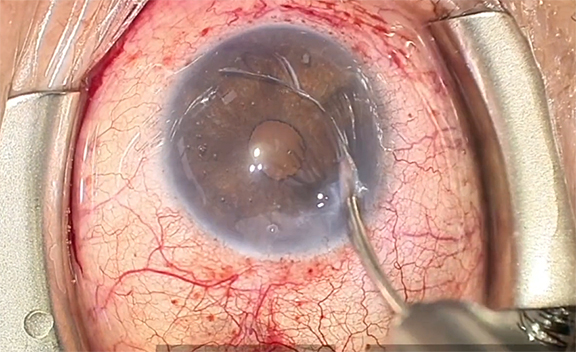
We're going about 2 millimeters from the limbus and entering parallel to the iris, and it's important that the needle is marked so that the entry site is visible. On removal of the needle, we slide a little bit laterally so that the external ostium of the needle tract is enlarged.
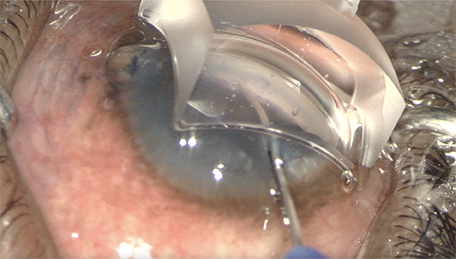
Here, we're deploying the Xen from the injector. We want to grab it about a third to 50% from the tip to allow us good control. We're adjusting the Xen again, and then we're placing it in that 30-gauge needle tract.
It's important to keep the stent dry. If it becomes wet, it's incredibly difficult to put into the tract that's been created and having that slightly enlarged opening does help on the external side.
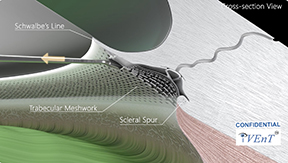
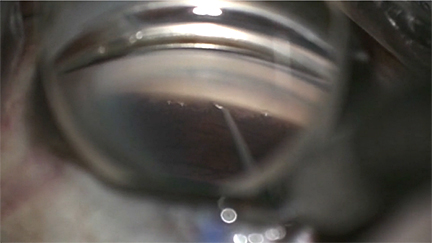
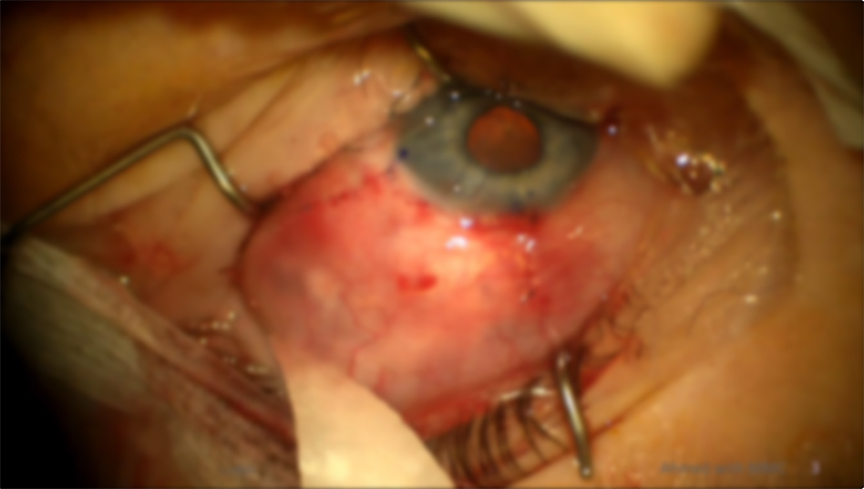
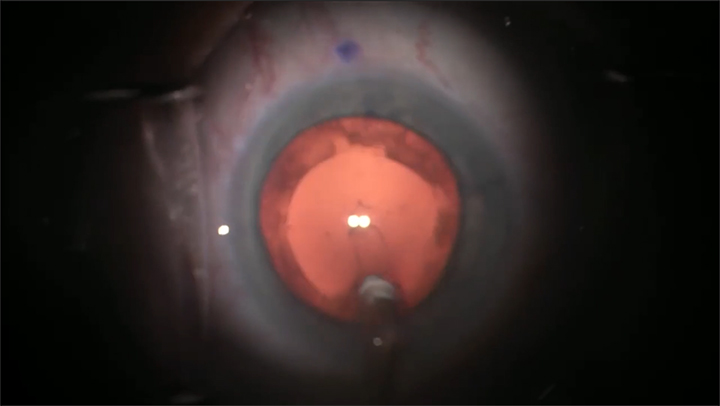
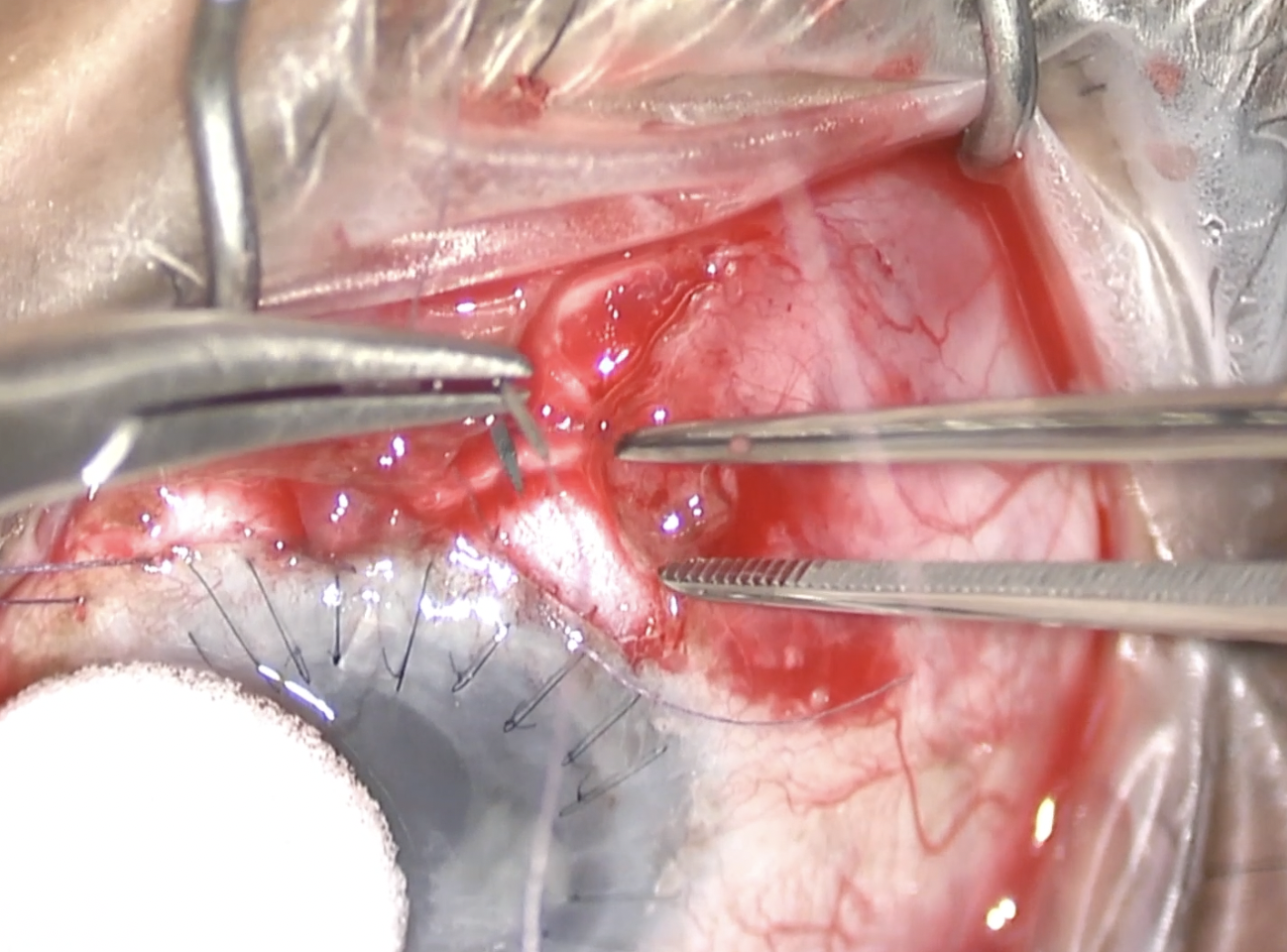
Here we're checking with the mirrored gonioprism to ensure that the stent is in good position and it's sitting right above the trabecular meshwork. Now we'll go to the closure. We like to close in 2 layers. The first layer we like to close is Tenons. Here we're grabbing Tenons and bringing it forward to make sure it'll sit nicely over the stent. Then we use a 9-0 Vicryl monofilament on a CS-160-8 needle. It's important that we check the stent to make sure it's straight in the sub-Tenon space without any kinks. Here, we're closing the first side of Tenons, and this knot does not need to be buried because it's going to be covered by conjunctiva. Then we'll close the other side of Tenons. Now all the fluid from the stent will flow into the sub-Tenon space where we applied that high-dose mitomycin, and this allows for a very posterior and diffuse bleb. Again, we're finishing the closure of the second side of Tenons. We then close the conjunctiva with a wing suture in a buried fashion again with the 9-0 Vicryl on the CS-160-8 needle.
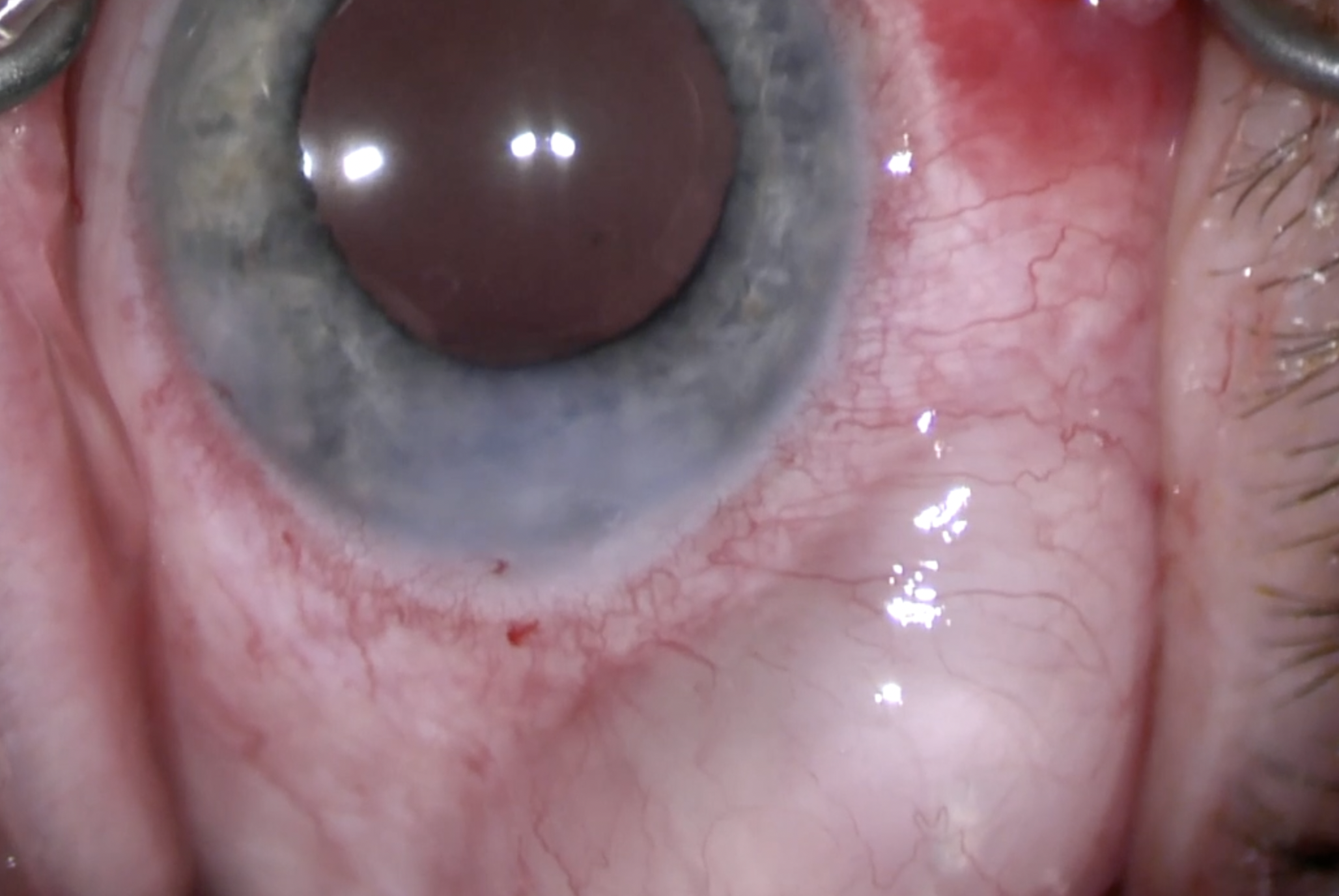
It's nice to have that bleb in the posterior sub-Tenon space, because the bleb morphology is a bit better than more anterior blebs that you see that are in the subconjunctival space. We close the radial incision with a horizontal mattress suture, then inject moxifloxacin intracamerally with a 30-gauge needle.

Other Videos From Series