For Glaucoma Physician's Surgical Pearls video series, Aaki Shukla, MD, and Ari Leshno, MD, demonstrate management of a case of a thin trabeculectomy flap. Transcript of the narration follows below.
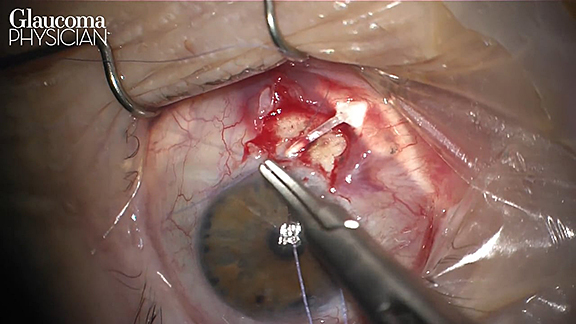
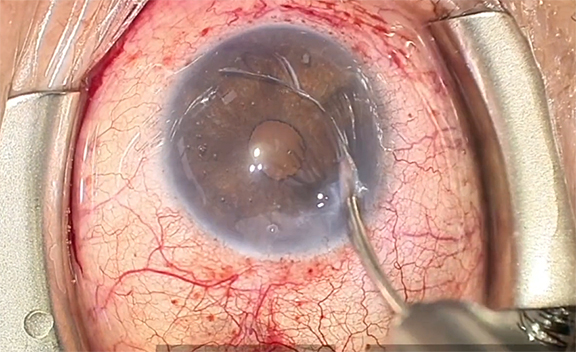
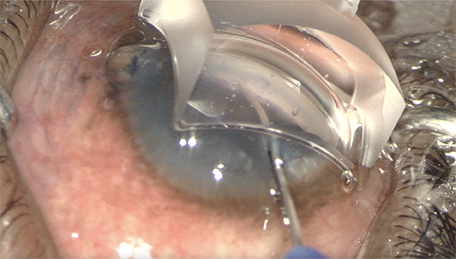
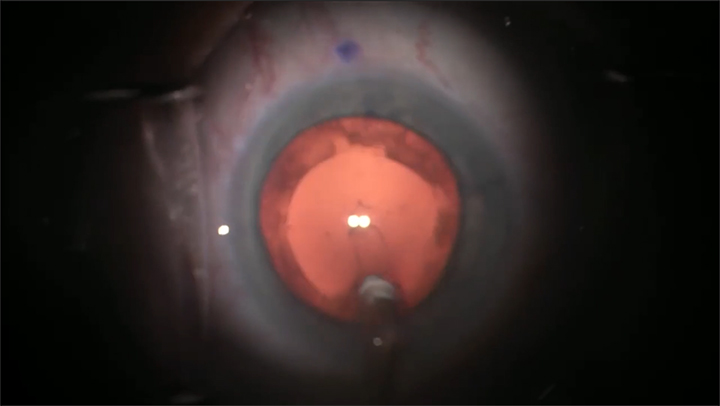
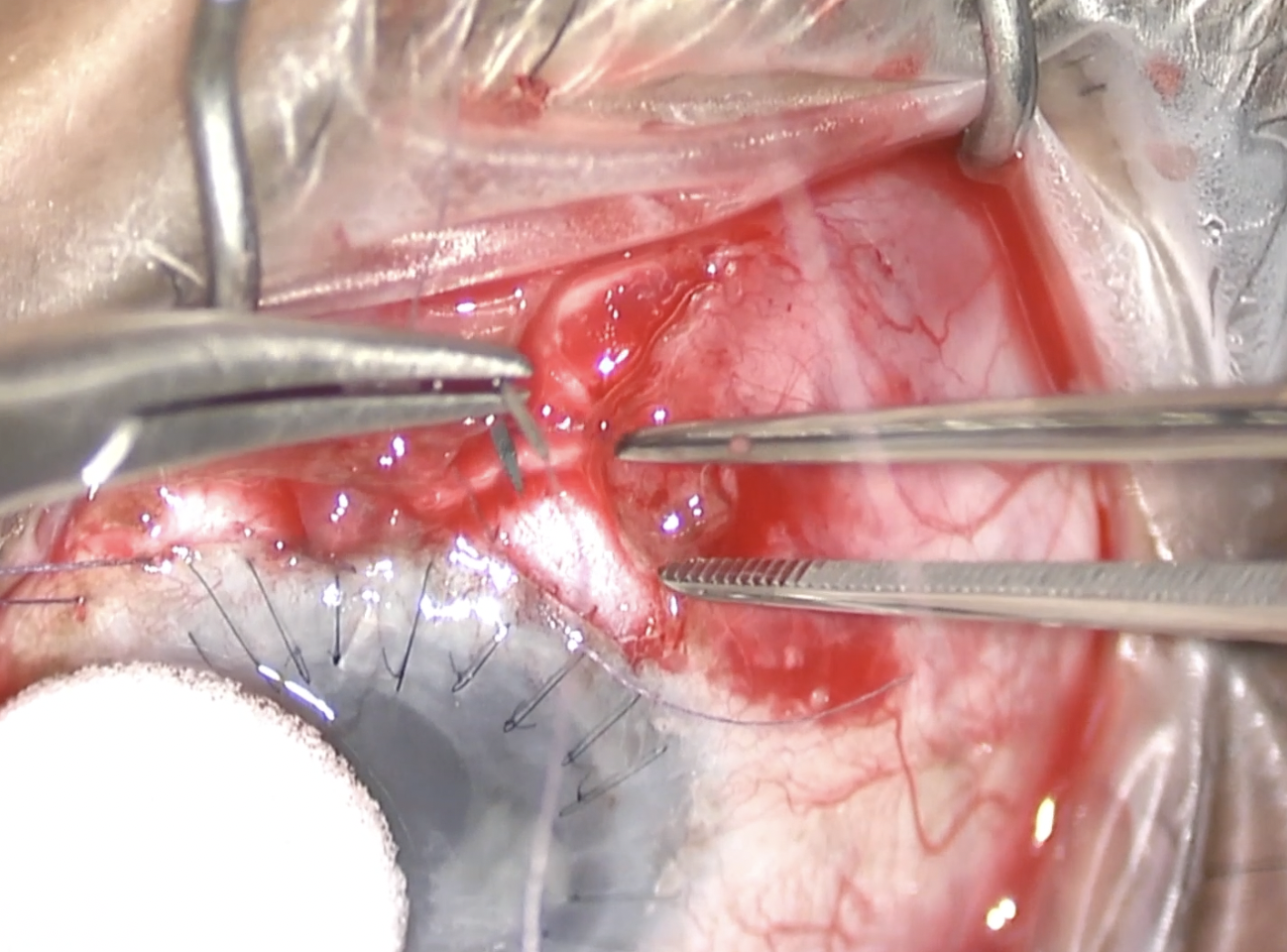
This is a 56-year-old woman undergoing trabeculectomy surgery. We are outlining the flap using a Supersharp blade. Then we use a crescent blade to create the flap. We try to remain in one plane. You can see that the right side of the flap has a weakness in it and there’s a depression where the flap is being grabbed by the Hoskins forceps centrally.
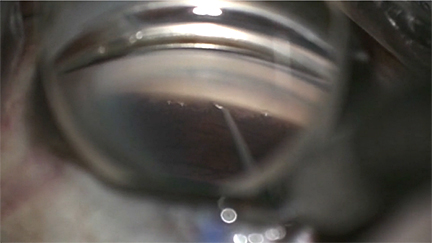
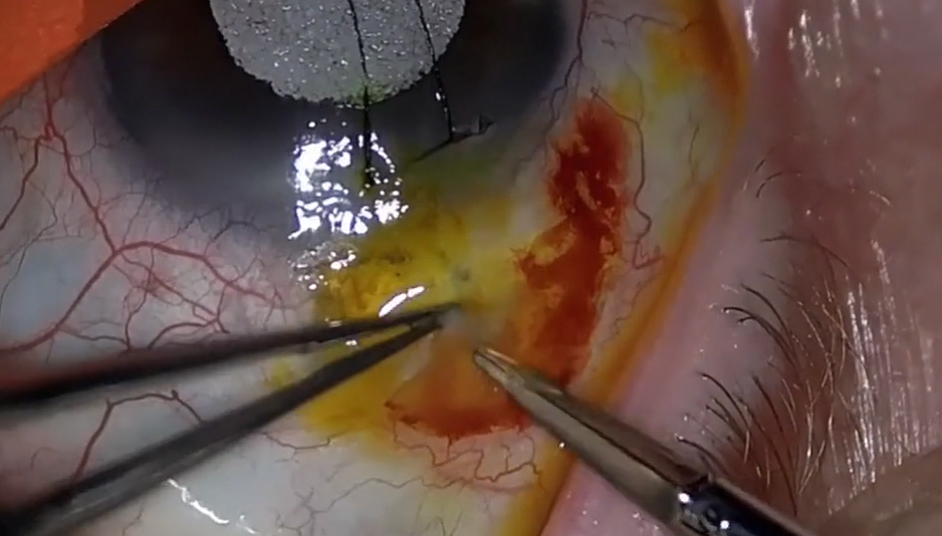
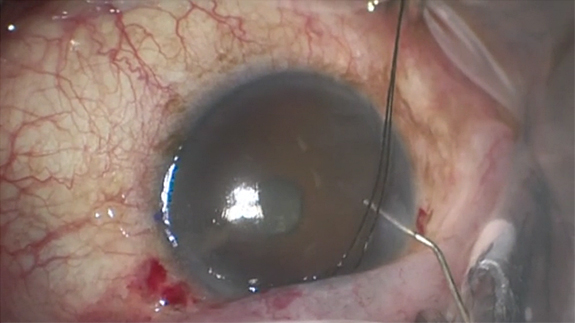
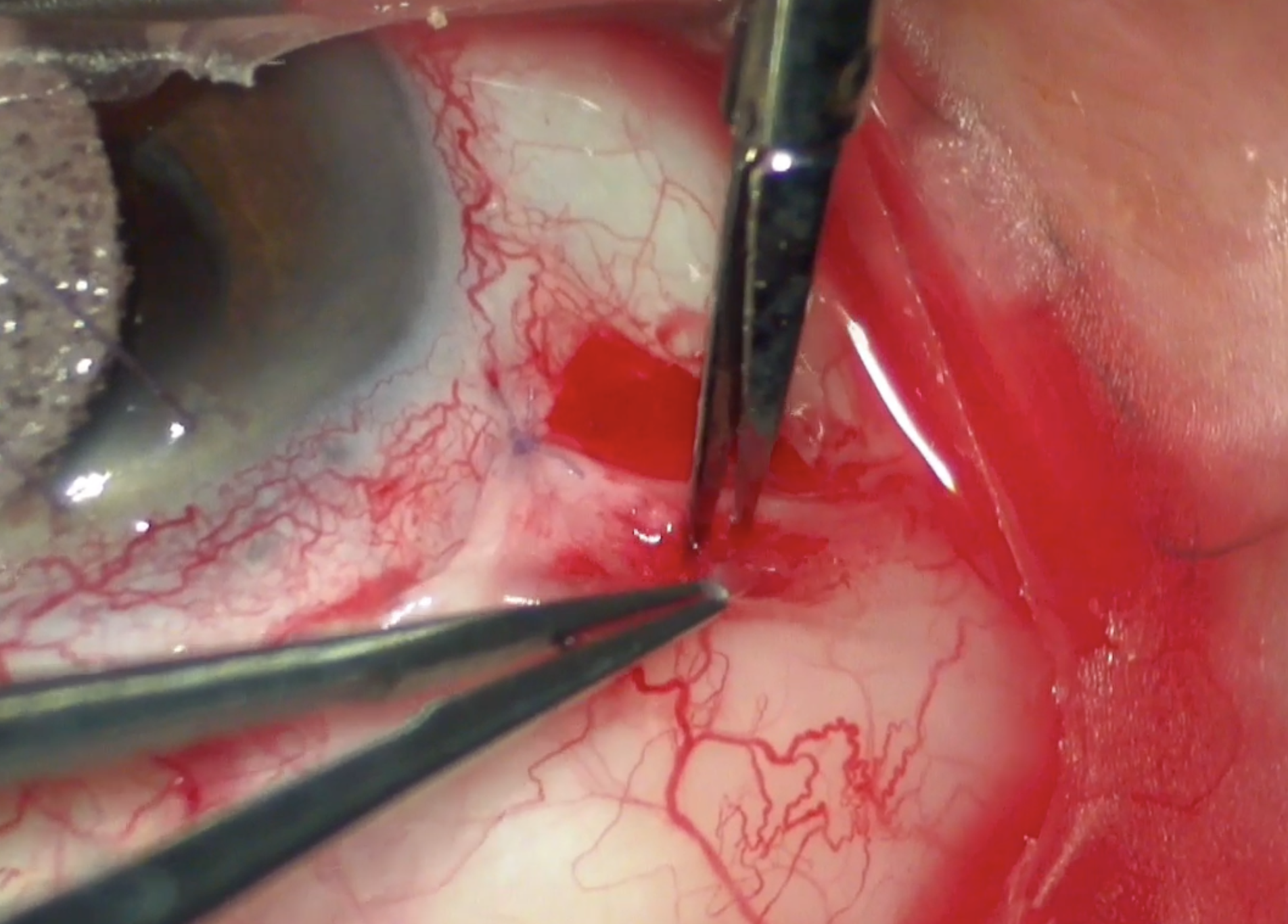
While we are preplacing the 10-0 nylon sutures, our traction suture unfortunately detaches at just the right time. We replace the traction suture and resume placing the nylon sutures. We unfortunately make multiple unnecessary needle passes while doing so. We enter the AC, make our sclerostomy site, and tie off our pre-placed sutures. But then we notice a leak where it appears that the flap has not reapproximated well, probably due to the weakness we had mentioned previously. We decide to place a suture in a leaky part of the flap, but then we saw a new leak on the other side of the flap. There was no denying it, so we place another suture on the other side. This resulted in a gush of fluid centrally, and we could confirm now that there was a hole in the center of the flap. This was likely from the multiple needle passes and sutures on each side that had gaped the opening.
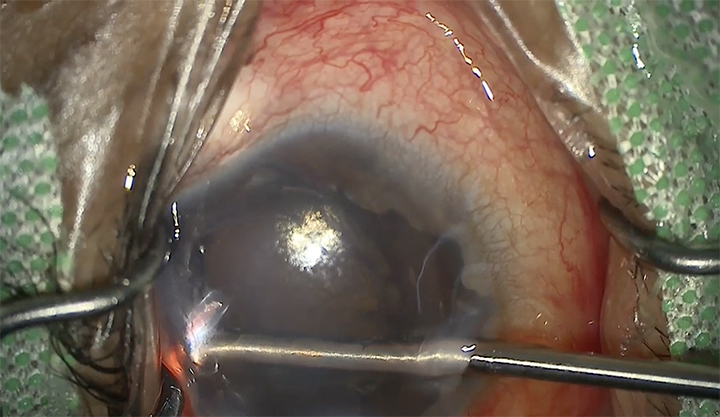
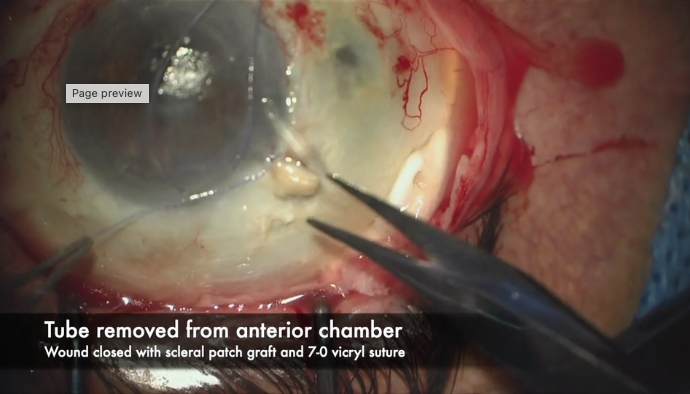
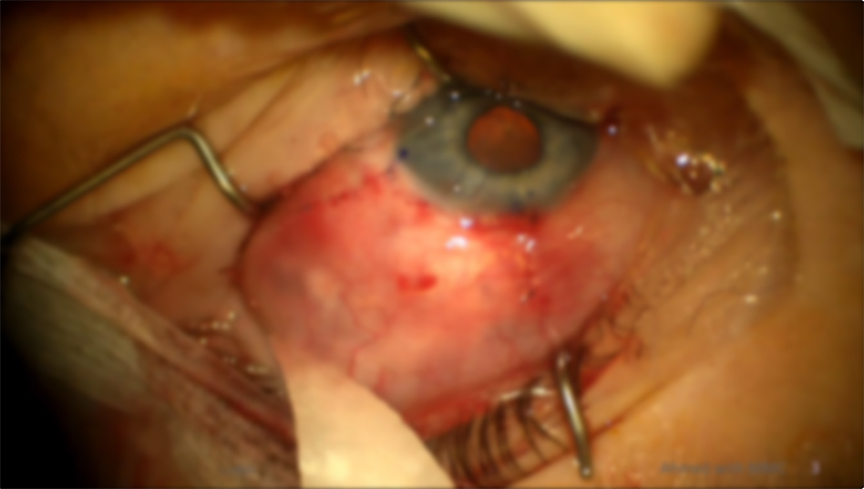
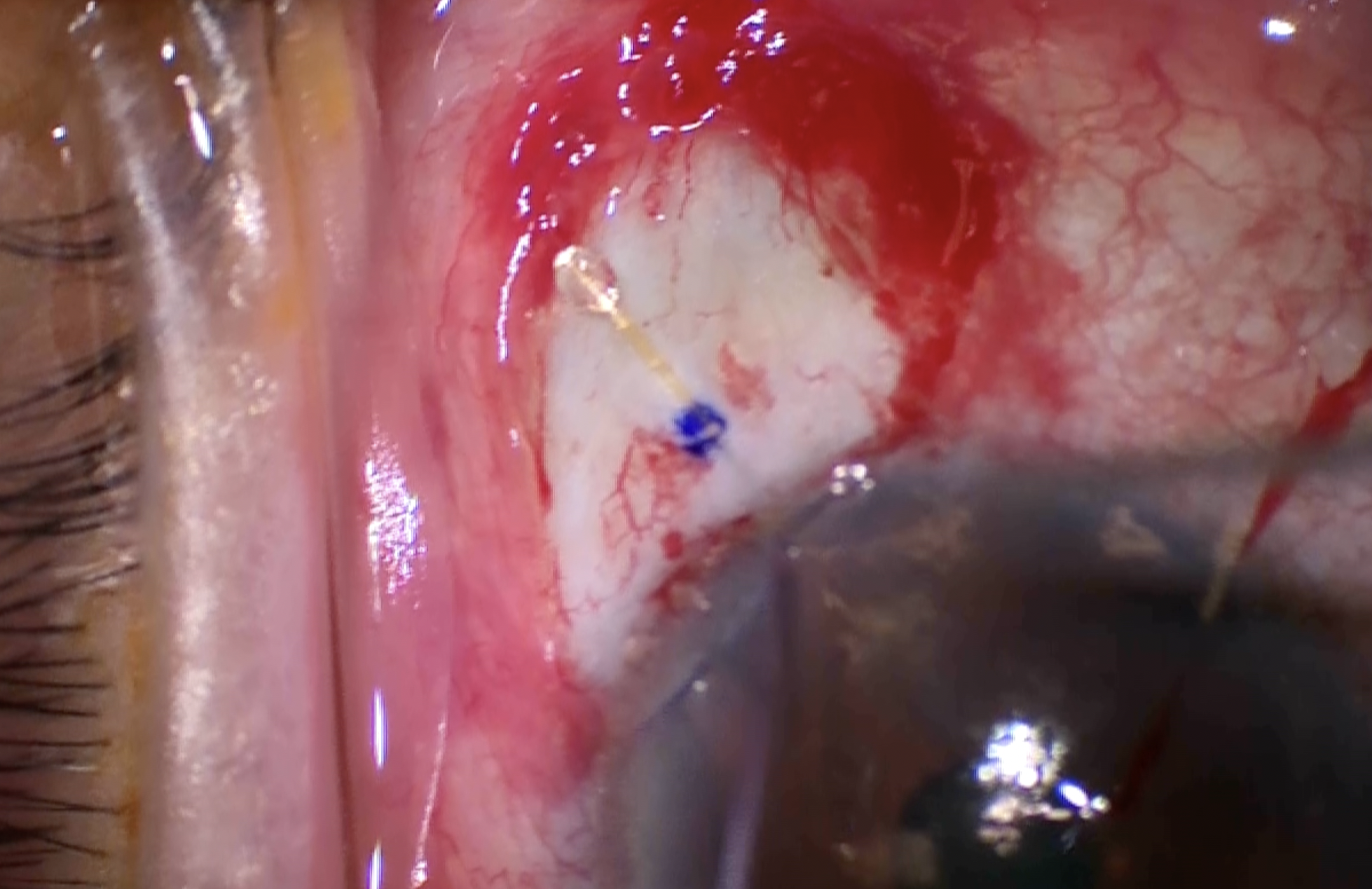
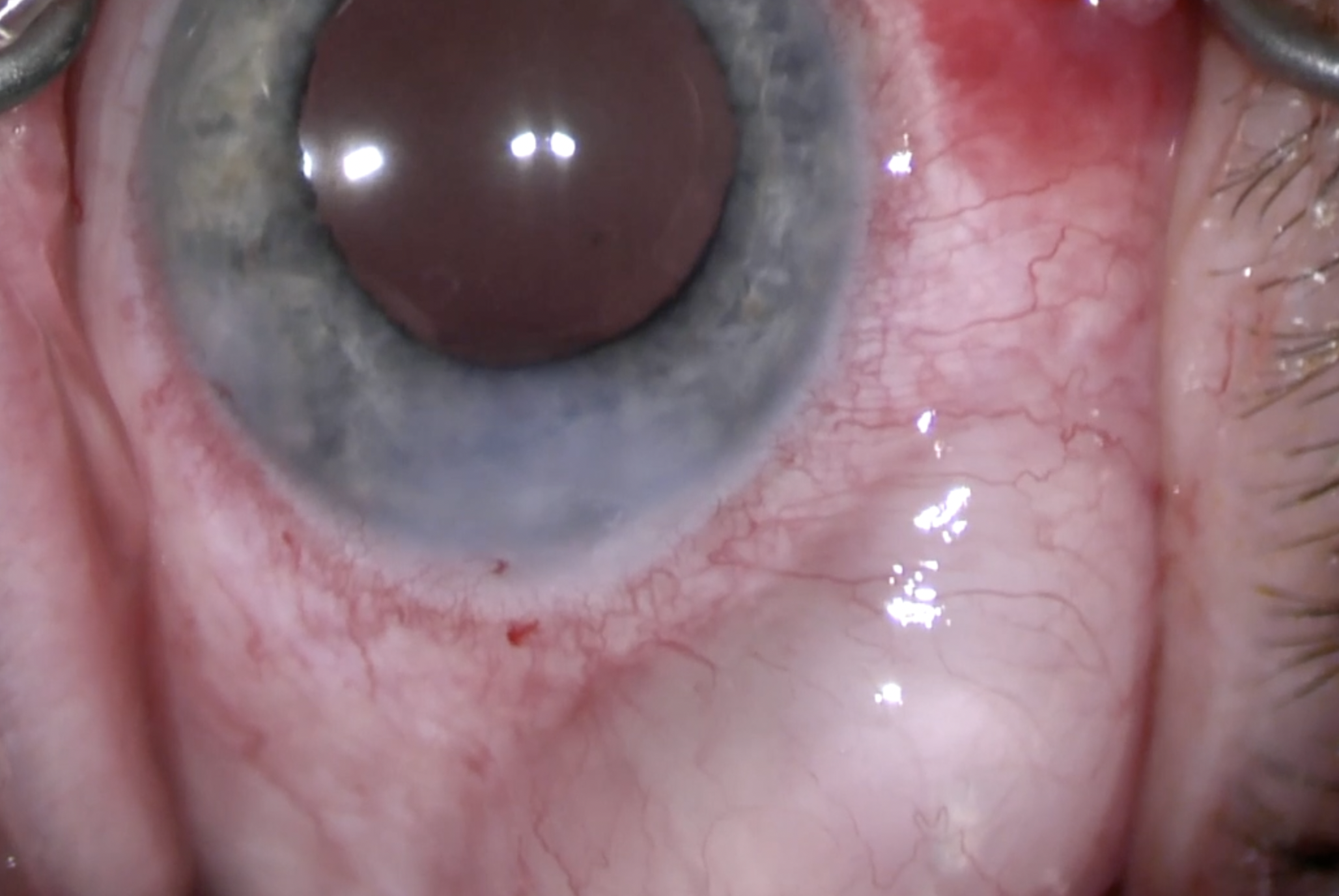
The cornea came to the rescue. We trimmed a piece of split-thickness half-moon VisionGraft and placed it over the leaking flap. We tied this off with 7-0 vicryl suture. We also trimmed it to promote posterior flow. We closed the peritomy with a central mattress and 2 winged sutures, all with 10-0 vicryl. At the end with had a deep AC and a watertight elevated bleb.
The pearls here are that if you notice that your trab flap is too thin pre-sclerostomy, you can abandon that site and start elsewhere. If you notice this post-sclerostomy, consider using a graft like we did. Avoid multiple needle passes, excessive cautery, flap creation in multiple planes, holding the flap with toothed forceps, and regrabbing the flap. Thanks for the opportunity to share this case with you and reach out to us with any questions.


Other Videos From Series