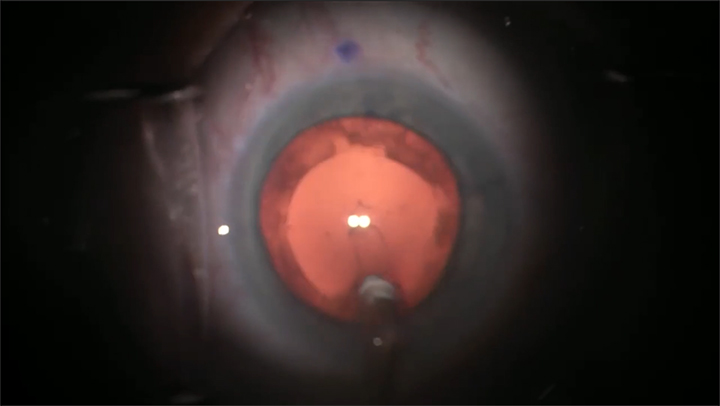
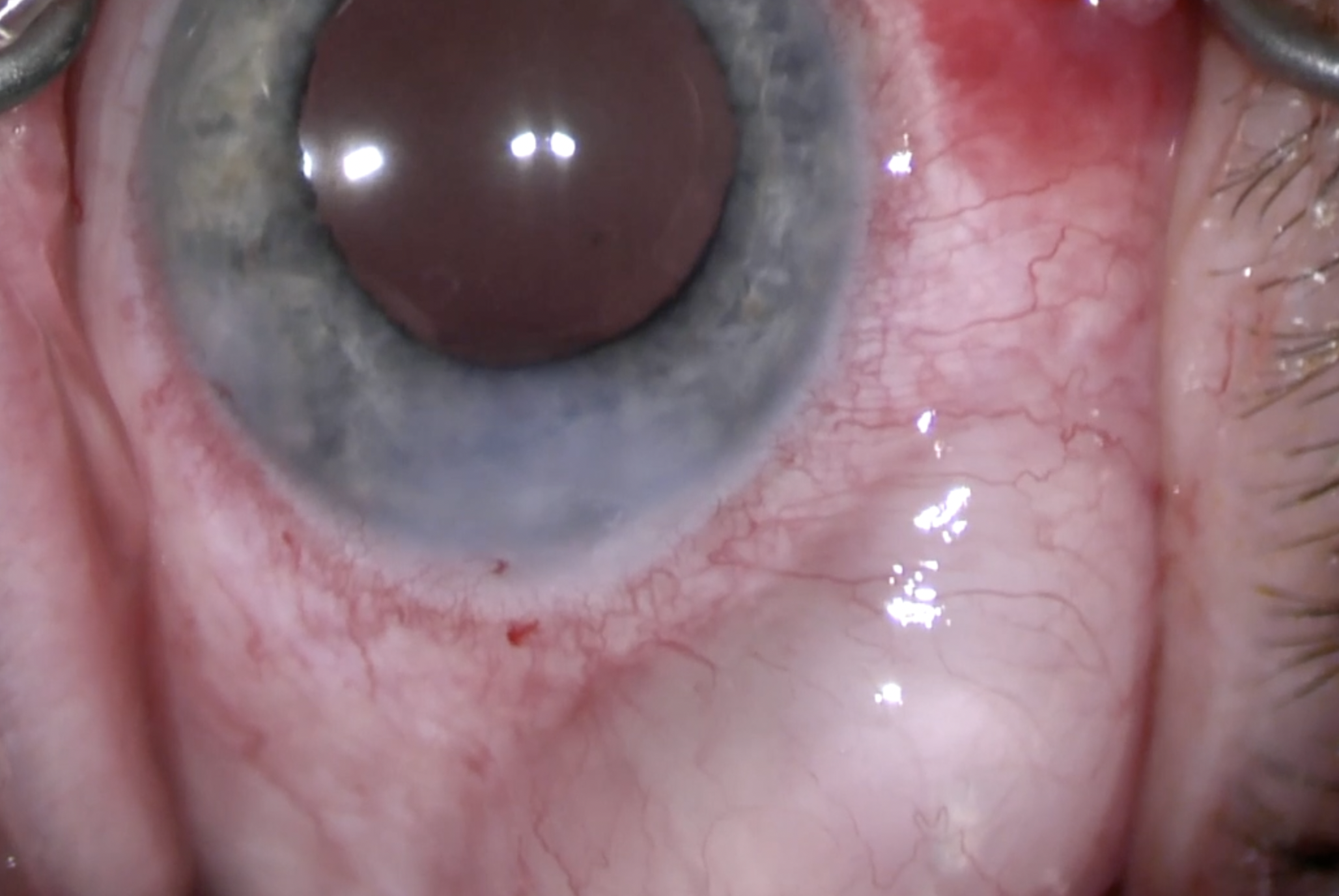
This is a case of a 90-year-old patient with uveitic glaucoma secondary to sarcoidosis presenting with her second glaucoma drainage implant erosion. Given the patient’s health status and poor visual potential of the eye, the decision was made to re-cover the shunt. We demonstrate a technique for repairing an erosion using fresh full thickness donor cornea tissue. After appropriately dissecting the conjunctiva, the graft is prepared and sized to provide maximum coverage. The graft is then sutured to the sclera, and the conjunctiva is reapproximated. Below is the transcript of this surgical video.
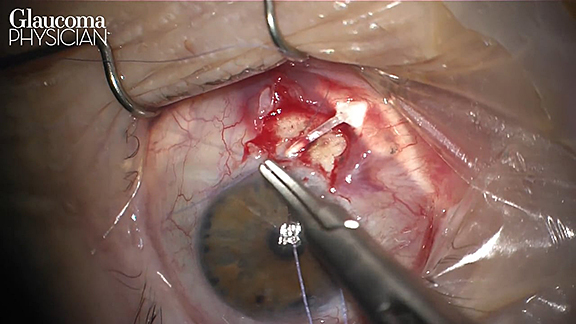
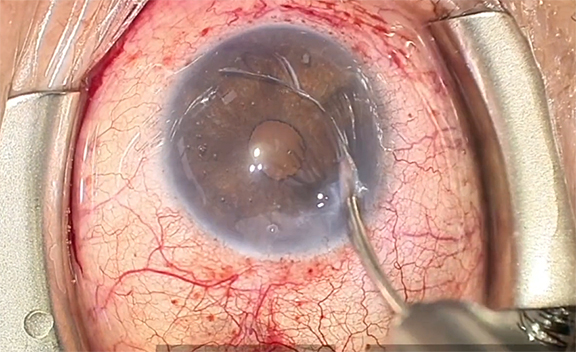
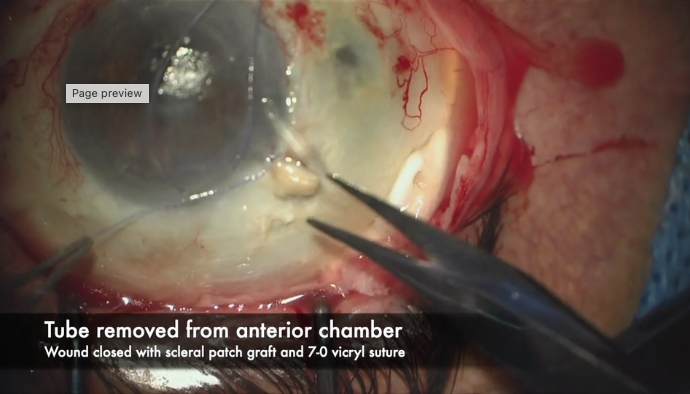
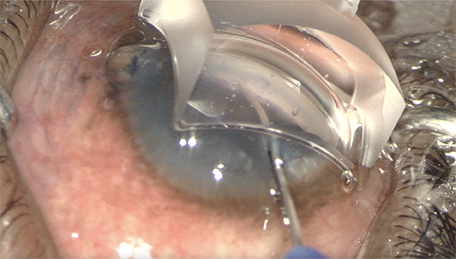
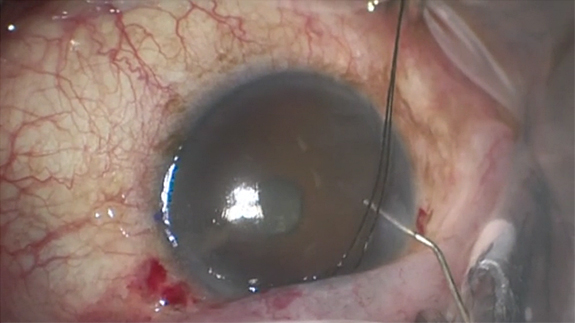
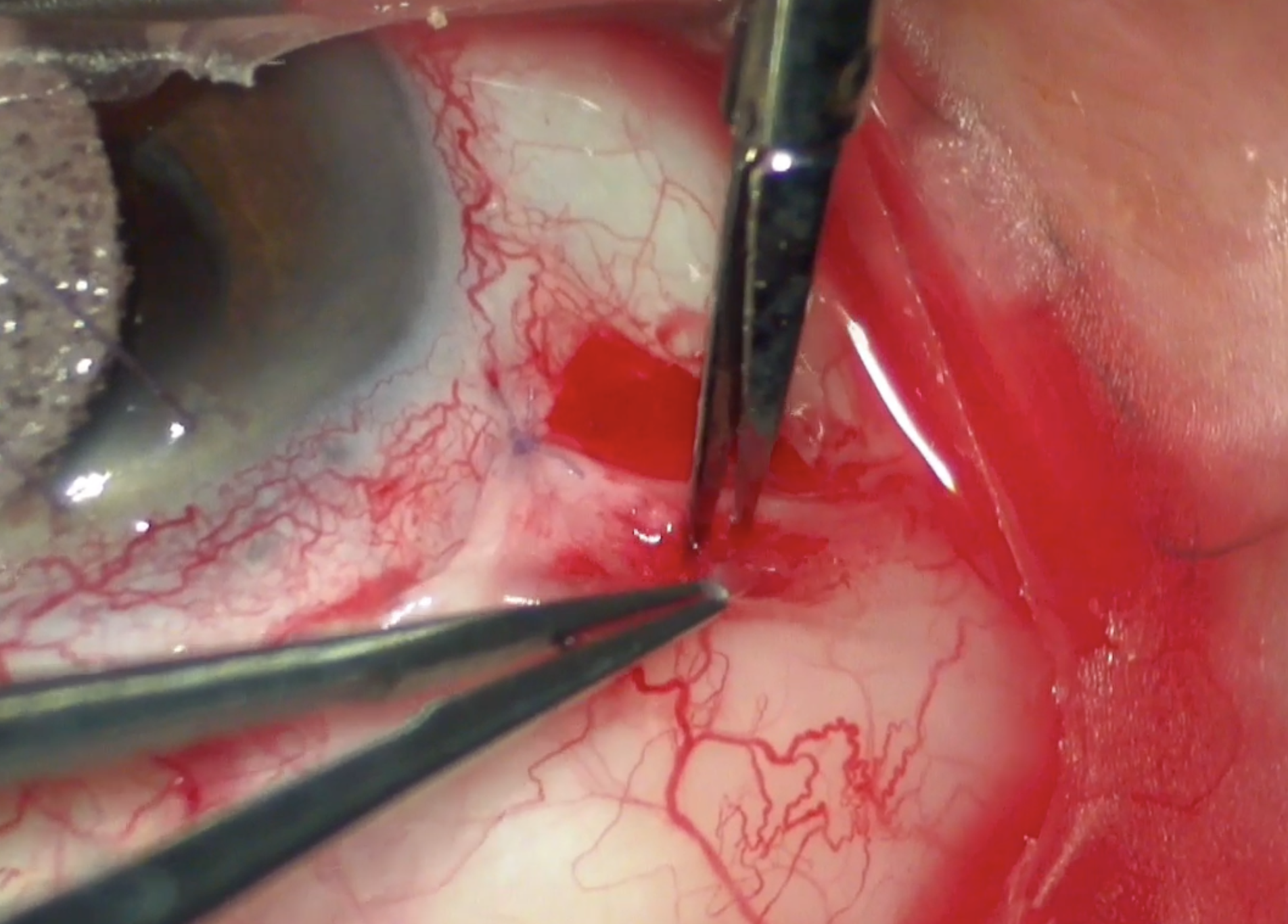
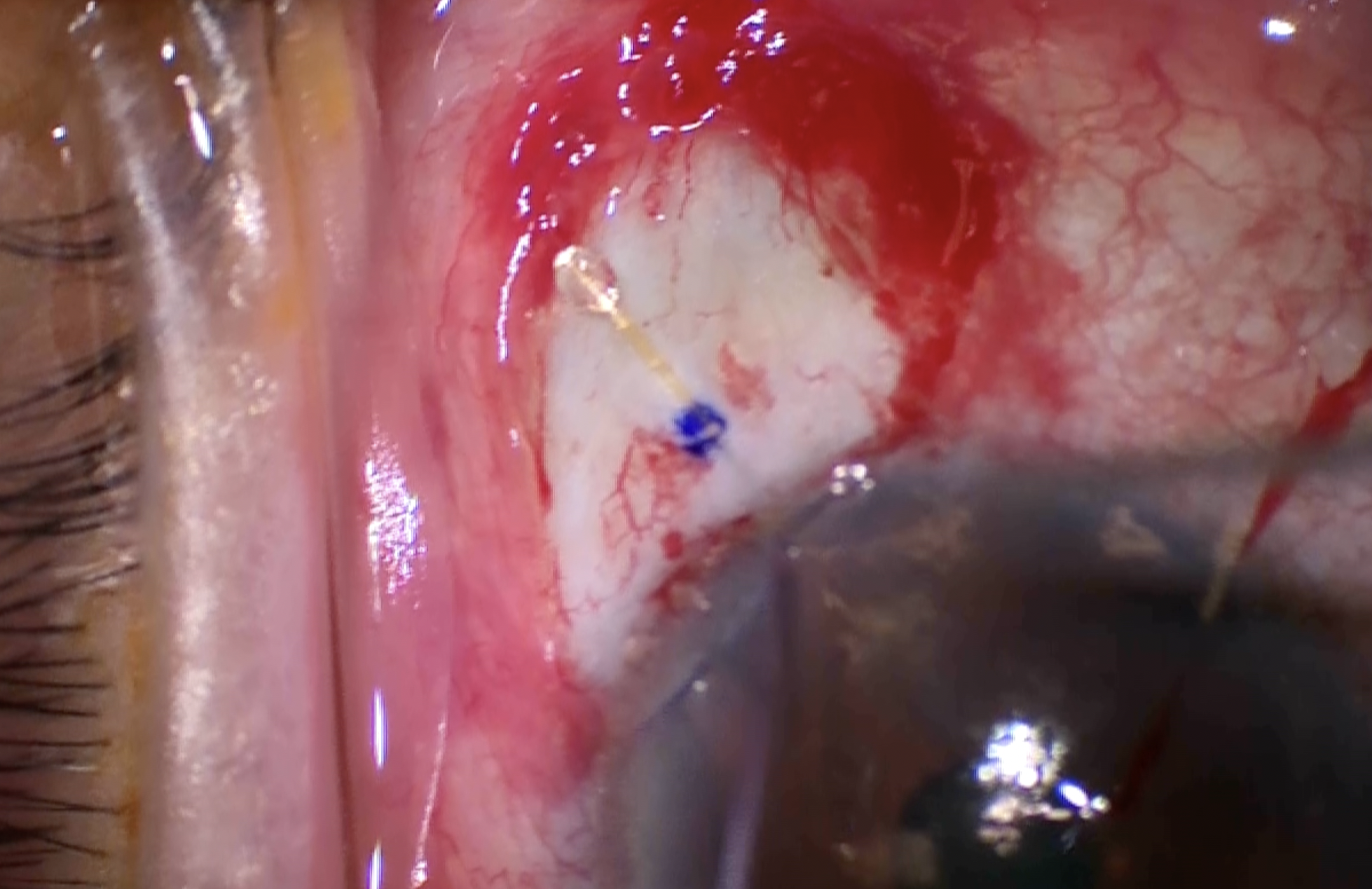
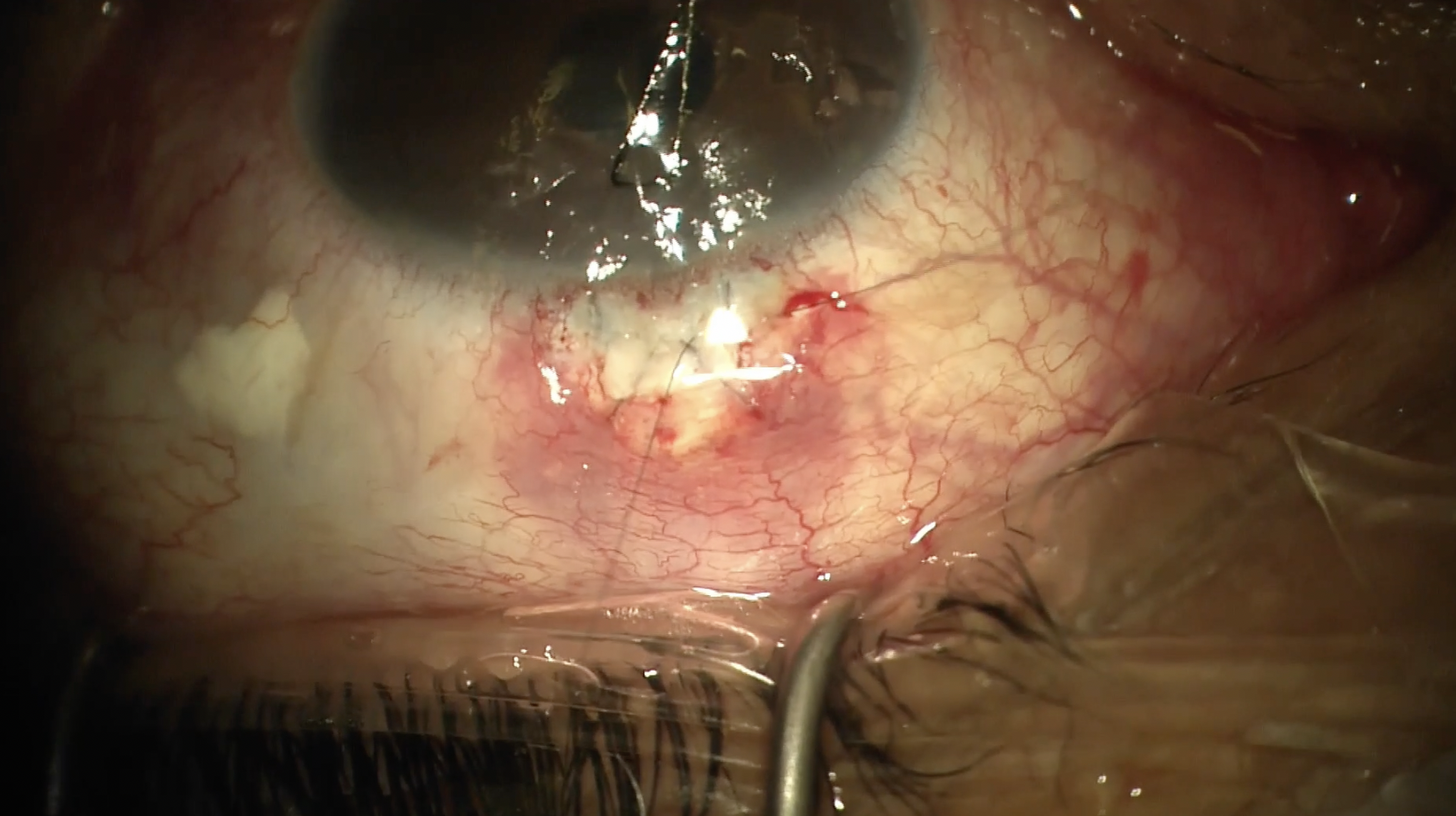
This is Ankur Parikh from the University of Cincinnati with Aubrey Tirpack as the operating surgeon, and this case demonstrates repair of a recurrent tube shunt erosion in a patient with uveitic glaucoma and a full thickness corneal transplant on chronic topical steroids. The case begins with a 7-0 vicryl corneal stay suture to expose the superotemporal quadrant, followed by dissection with blunt Westcott scissors and tissue forceps to expose the tube shunt, taking care not to disinsert the tube from the anterior chamber. Next, we prepare our full-thickness fresh donor cornea using a #15 blade and 0.12 forceps to strip Descemet’s membrane and resize to the appropriate length. Then we use 8-0 vicryl on a TD-140 needle to secure the corneal graft to the sclera with four simple interrupted sutures. We make sure to undermine the posterior conjunctiva to fully tuck the graft in and cover as much of the tube as possible.
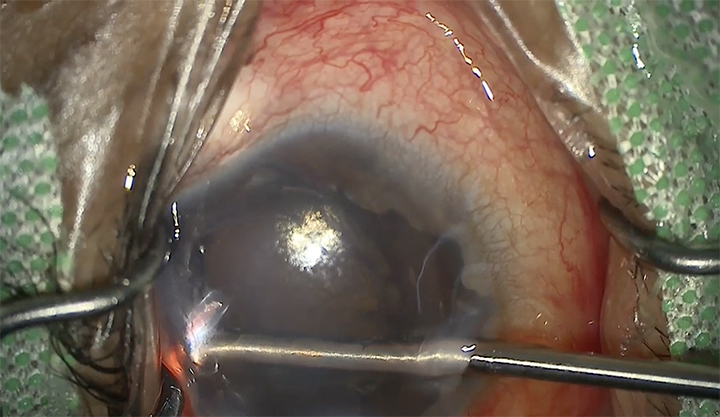
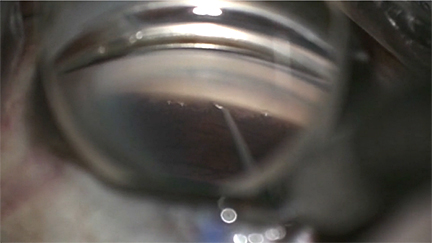
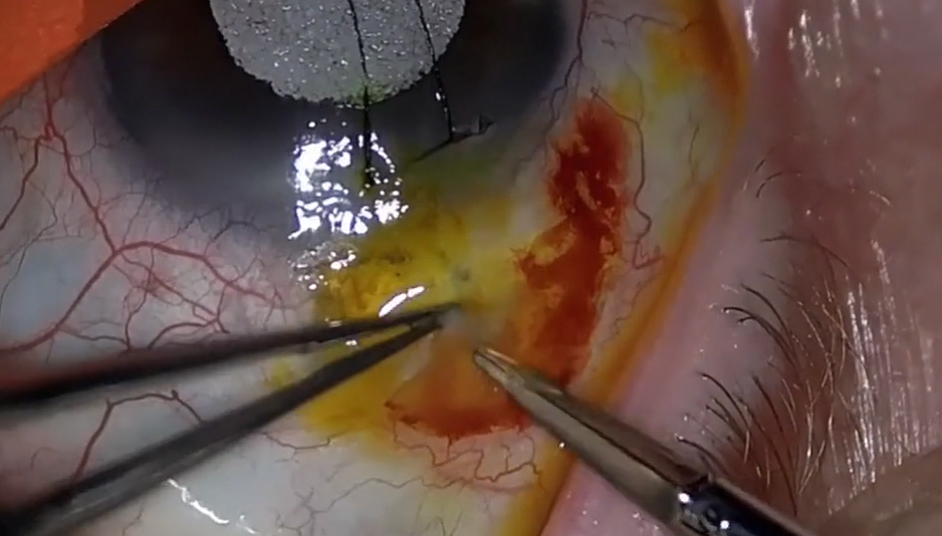
Here, we are approximating the conjunctiva to ensure there is enough tissue for a complete closure. Now, we shave the anterior portion of the graft to minimize override on the peripheral cornea. Then, with our same 8-0 vicryl, we take a radial bite and secure the anterior portion of the graft to the limbus using a mattress suture. This is important as the anterior portion of the graft is a frequent site of recurrent erosion. Finally, we begin our closure.
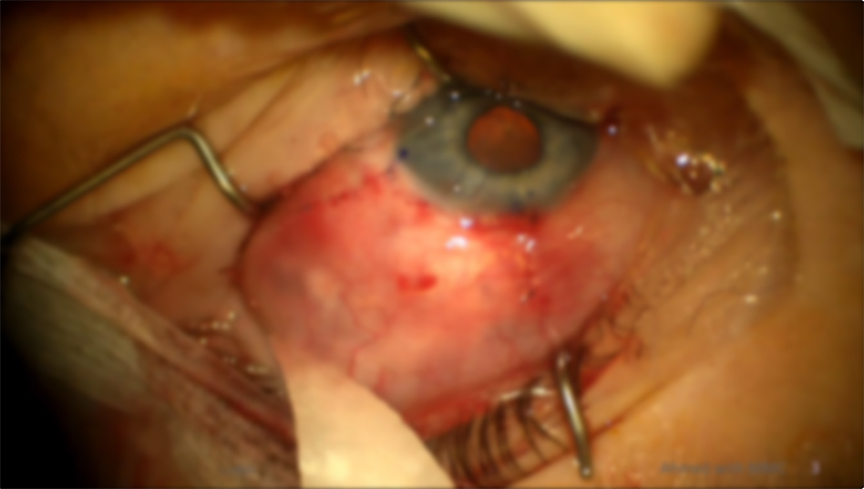
We start by once again approximating the conjunctiva to the limbus to ensure we have enough free tissue. With the same 8-0 vicryl and horizontal mattress technique, we secure the conjunctiva to the episclera on top of the patch graft. For the peripheral portions of the closure, simple interrupted passes from the episclera to the conjunctiva are sufficient. The last step is a simple running suture to close the remainder of the conjunctiva posteriorly After completion of the closure, the corneal stay suture was removed, and the patient was given subconjunctival injections of dexamethasone and Ancef. They were discharged with moxifloxacin and prednisolone forte drops to be used 4 times a day.
Thank you for watching this video, we hope you will consider this technique when repairing glaucoma drainage implant erosions. Please email Dr. Tirpack with any questions.

Other Videos From Series